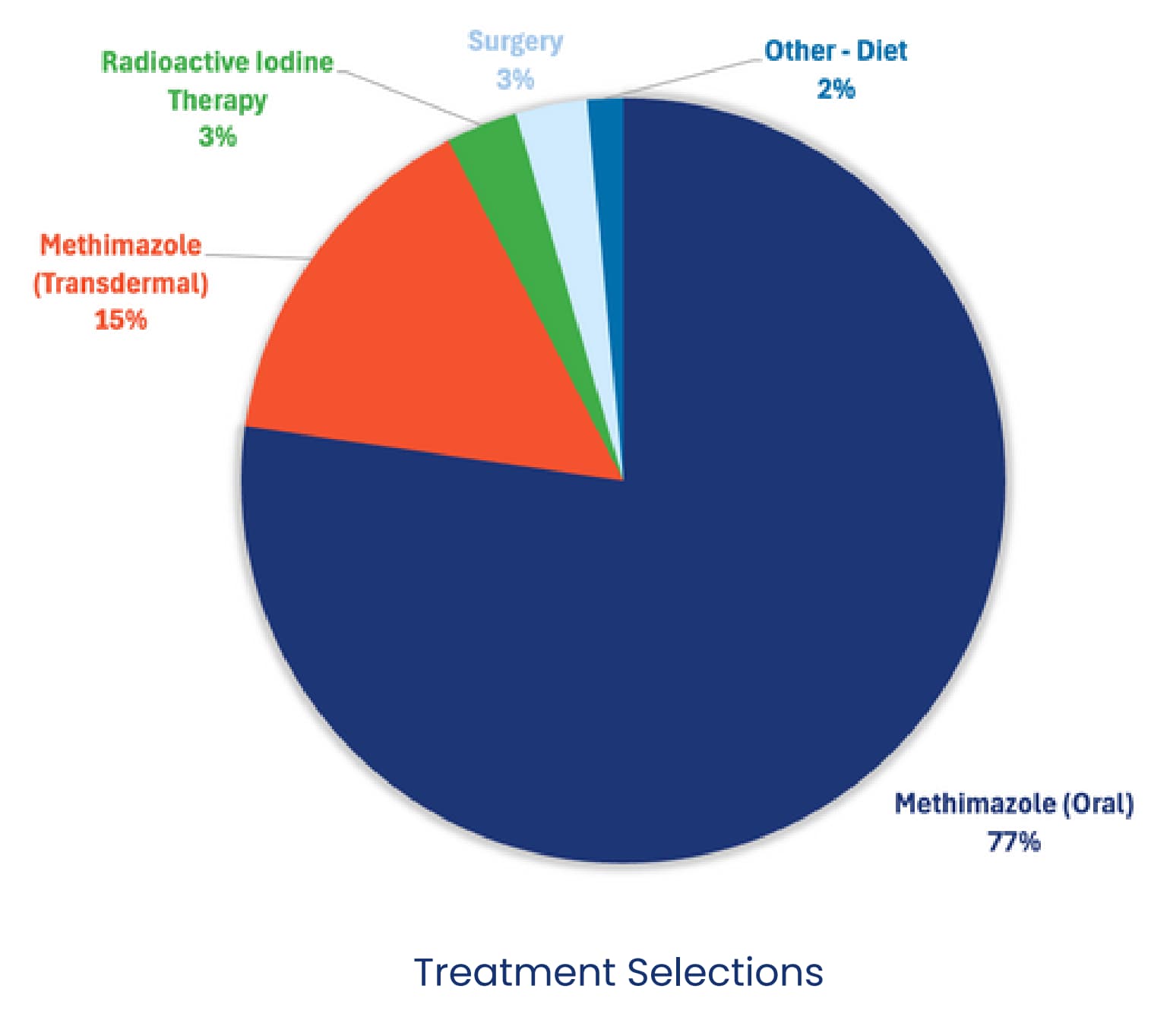
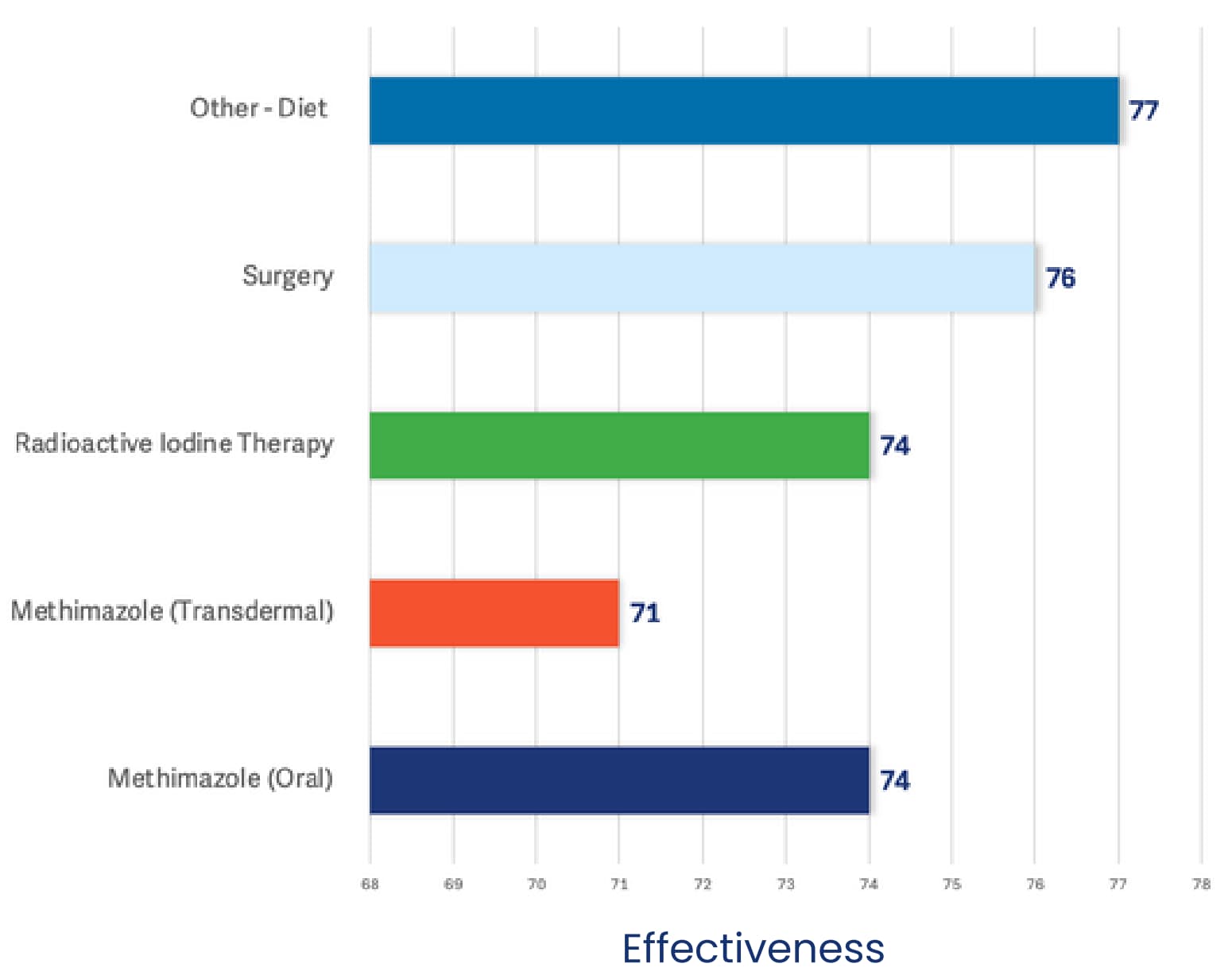
Among responding DVMs, 77% identified oral methimazole as their first-line treatment for feline hyperthyroidism, and those who used it reported effectiveness in more than 74% of their cases.

Feline Hyperthyroidism
Specialists Insight
1. Radioactive Iodine Therapy (I-131) – The Gold Standard
Most veterinary endocrinologists consider I-131 the gold standard. It destroys abnormal thyroid tissue while preserving healthy cells and is usually curative with a single treatment. A short hospitalization (3–5 days in the U.S.) is required for radiation safety.
Success Rate:
- 94–98% cure rate with one dose
- Rare recurrence if all abnormal tissue is destroyed
Pros: Permanent cure, no daily medication, minimal side effects Cons: Higher upfront cost, limited availability, temporary owner separation
Cons: Higher upfront cost, limited availability, temporary owner separation
2. Surgical Thyroidectomy – A Curative Option When I-131
Recommended for otherwise healthy cats when I131 is not available or declined. Pre-op stabilization with methimazole is essential. Surgery can be unilateral or bilateral depending on gland involvement.
Success Rate:
- 90–98% long-term cure if both abnormal lobes are removed and no ectopic tissue is present
- Low complication rate, though hypocalcemia from parathyroid damage can occur
Pros: Potential cure, no long-term medication
Cons: Anesthesia/surgical risk, possible recurrence if tissue is missed, lifelong monitoring if hypocalcemia develops
3. Medical Management (Methimazole) – Control Without Cure
Best for cats that aren’t surgical or I-131 candidates, or for owners preferring a non-curative approach. Can be given orally or transdermally. Controls the disease but does not stop tumor growth.
Success Rate:
- 80–90% achieve good hormone control with proper dosing and monitoring
- Long-term control possible for years if well tolerated
Pros: Inexpensive short-term, widely available, reversible if side effects occur
Cons: Lifelong treatment, potential side effects (GI upset, pruritus, liver toxicity, blood dyscrasias), frequent monitoring needed