This is a network committed to advancing clinical understanding through real-world outcomes. We believe veterinarians hold unparalleled insight into what truly works in practice. Each week, we pose one focused clinical question to the veterinary community. On Mondays, we present the question. On Fridays, we share your responses—highlighting the treatments and protocols delivering the best outcomes. Together, we’re building a living library of frontline veterinary wisdom.
CLINICAL PERSPECTIVE
This Week’s Sticky Case
Patient
11-year-old Spayed Female Golden Retriever
Presenting Complaint
Acute onset head tilt and inability to stand
History
The owner reports that the dog woke up this morning unable to walk normally.
Additional history includes:
- Normal behavior the previous evening
- Acute onset of head tilt overnight
- Two episodes of vomiting this morning
- No known trauma
- No seizure history
- Appetite normal until this morning
- Vaccinations current
- Monthly preventatives current
Physical Examination
- Quiet but responsive
- Temperature: 101.9°F
- Heart Rate: 92 bpm
- Respiratory Rate: 24 bpm
- Pronounced right head tilt
- Horizontal nystagmus present at rest
- Unable to maintain balance without assistance
- Delayed proprioception in the right thoracic limb
- Mentation mildly obtunded
- Cranial nerve examination otherwise unremarkable
Diagnostics
CBC
Within normal limits
Serum Chemistry
No significant abnormalities
Blood Pressure
Normal
Thoracic radiographs previously performed six months ago were unremarkable.
Provide Your Clinical Insight
Last Week’s Results
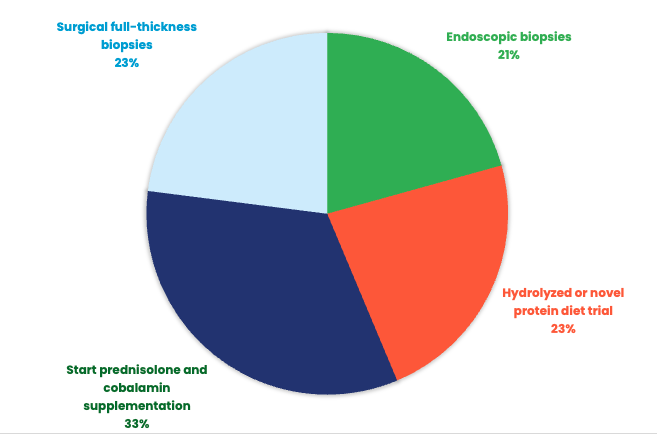
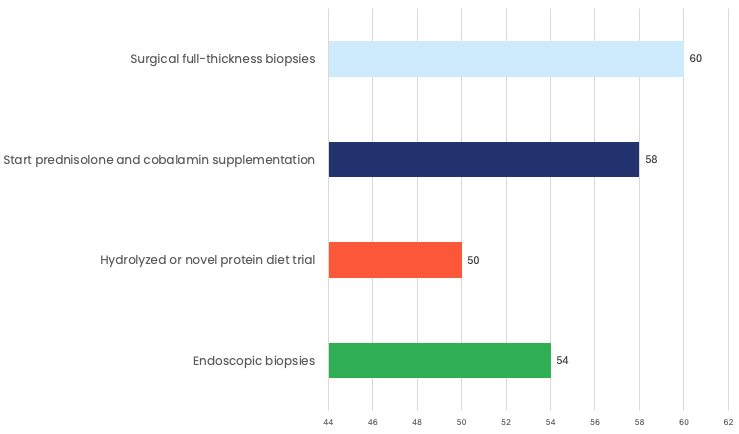
This week’s survey results showed a fairly even split across diagnostic and treatment approaches, highlighting how nuanced chronic GI cases can be in general practice. The largest group of respondents, 33%, selected starting prednisolone and cobalamin supplementation, suggesting many clinicians are thinking about inflammatory disease management and supportive care early in the process.
Two options tied closely behind, with 23% selecting a hydrolyzed or novel protein diet trial and another 23% choosing surgical full-thickness biopsies. This reflects the balance many veterinarians face between pursuing a less invasive therapeutic trial and moving toward more definitive diagnostics. Endoscopic biopsies followed closely at 21%, showing strong consideration for minimally invasive tissue sampling when available.
Overall, the results point to a common clinical crossroads: deciding when to treat empirically, when to pursue diet trials, and when tissue diagnosis is needed to guide the next step.
Responding DVMs were asked to identify their next step in the presented case. Over 58% of the responding DVMs selected an abdominal ultrasound as their next step. The specialists agree. Read more to learn why.
CLINICAL PERSPECTIVE
How would you handle the case?
How a General Practitioner Might Approach This Case
This is one of the most challenging feline GI presentations encountered in practice because the likely diagnoses are familiar, but the next step is not always obvious.
At first glance, the patient appears relatively stable:
- Good appetite
- Mild clinical signs
- No severe biochemical abnormalities
- No obvious intestinal mass
Many veterinarians would understandably consider initiating prednisolone and cobalamin supplementation.
After all, inflammatory bowel disease is common, cobalamin deficiency is present, and many cats experience clinical improvement with empirical therapy.
The challenge is that this case sits squarely in the gray zone between chronic enteropathy and small-cell intestinal lymphoma.
And those two diseases can look remarkably similar.
How Specialists Typically View This Case
From an internal medicine perspective, the most appropriate next recommendation is:
Endoscopic Biopsies
The reason is not that specialists disagree with treating inflammation.
The reason is that specialists want to know exactly what they are treating before initiating therapy that may alter the diagnostic landscape.
Why Biopsy Becomes Important
Several findings in this case raise concern beyond uncomplicated inflammatory bowel disease:
- Progressive weight loss
- Muscle wasting despite a good appetite
- Low cobalamin concentration
- Intestinal muscularis thickening
- Mild lymph node enlargement
- Advanced age
Collectively, these findings create significant overlap between two common feline diseases:
Chronic Inflammatory Enteropathy
and
Small-Cell Intestinal Lymphoma
Unfortunately, clinical signs, laboratory findings, and even ultrasound changes frequently overlap between these conditions.
The question is no longer:
“Does this cat have gastrointestinal disease?”
The question becomes:
“Is this inflammatory disease, neoplastic disease, or both?”
That distinction has direct implications for treatment recommendations, prognosis, and long-term monitoring.
Why Not Start Prednisone First?
This is where many specialists diverge from general practice.
Prednisolone often improves both inflammatory bowel disease and small-cell lymphoma.
The problem is that improvement does not equal diagnosis.
Once corticosteroids are initiated:
- Histopathologic interpretation may become more difficult
- Lymphocyte populations may change
- Diagnostic yield may decrease
- Distinguishing lymphoma from inflammation becomes more challenging
In referral medicine, one of the most common frustrations is evaluating a cat after weeks or months of corticosteroid therapy have already been started.
While the patient may feel better, the opportunity to establish a definitive diagnosis may have been compromised.
Why Not a Diet Trial?
Diet trials remain a cornerstone of chronic enteropathy management.
However, specialists often become more aggressive diagnostically when additional risk factors emerge.
This patient has:
- Significant weight loss
- Muscle loss
- Ultrasound abnormalities
- Cobalamin deficiency
At this stage, many internists would argue the case has progressed beyond a simple dietary investigation.
A diet trial may ultimately become part of the treatment plan, but it is unlikely to answer the primary diagnostic question.
Why Endoscopic Instead of Full-Thickness Biopsies?
This is where the debate becomes particularly interesting.
Many specialists would begin with endoscopic biopsies because:
- The disease appears diffuse rather than focal
- No discrete mass lesions are identified
- Morbidity is lower
- Recovery is faster
- Diagnostic yield is often sufficient for chronic enteropathy and small-cell lymphoma
Full-thickness biopsies certainly provide more tissue architecture and deeper layers of the intestinal wall.
However, they carry greater procedural risk and are generally reserved for situations where:
- Endoscopic samples are non-diagnostic
- Focal lesions are identified
- Muscularis disease is strongly suspected
- Clinical suspicion remains high despite negative findings
This is one of the rare situations where even specialists may reasonably disagree.
The Bigger Clinical Question
One of the most important lessons in feline medicine is recognizing when empirical therapy is no longer enough.
Early in the course of chronic GI disease, diet modification and supportive care are often entirely appropriate.
As cases progress and objective abnormalities accumulate, the value of obtaining a definitive diagnosis increases substantially.
This patient has reached that threshold.
Specialist Takeaway
For this cat, most internists would recommend:
Endoscopic Biopsies
Not because treatment is inappropriate.
Not because prednisolone will not help.
But because establishing a diagnosis before initiating long-term immunosuppressive therapy provides the greatest opportunity to make informed decisions about treatment, prognosis, and monitoring.
The broader lesson is one that frequently emerges in referral medicine:
When weight loss, intestinal thickening, cobalamin deficiency, and lymph node changes begin to converge, the question shifts from how to manage the disease to understanding exactly which disease is present.
And in this case, tissue remains the issue.
Clinical Outcomes Annual Report
This report brings together the answers to more than fifteen of this year’s most important clinical questions, offering a comprehensive view of what is working in practices across the country.
Subscribe today and become part of the Clinical Outcomes Network.
Check Out Past Results
See how veterinarians nationwide answered previous Clinical Outcomes questions and what their results reveal.
2 Comments. Leave new
Love the result/pie chart!
Excellent resource