GDV is a true surgical emergency, but survival is strongly influenced by preoperative stabilization, control of shock, and rapid decompression. The goal is always the same: restore perfusion, relieve gastric pressure, and get to surgery quickly once the patient is stable enough for anesthesia.

Gastric Dilatation- Volvulus (GDV)
Treatment Selections
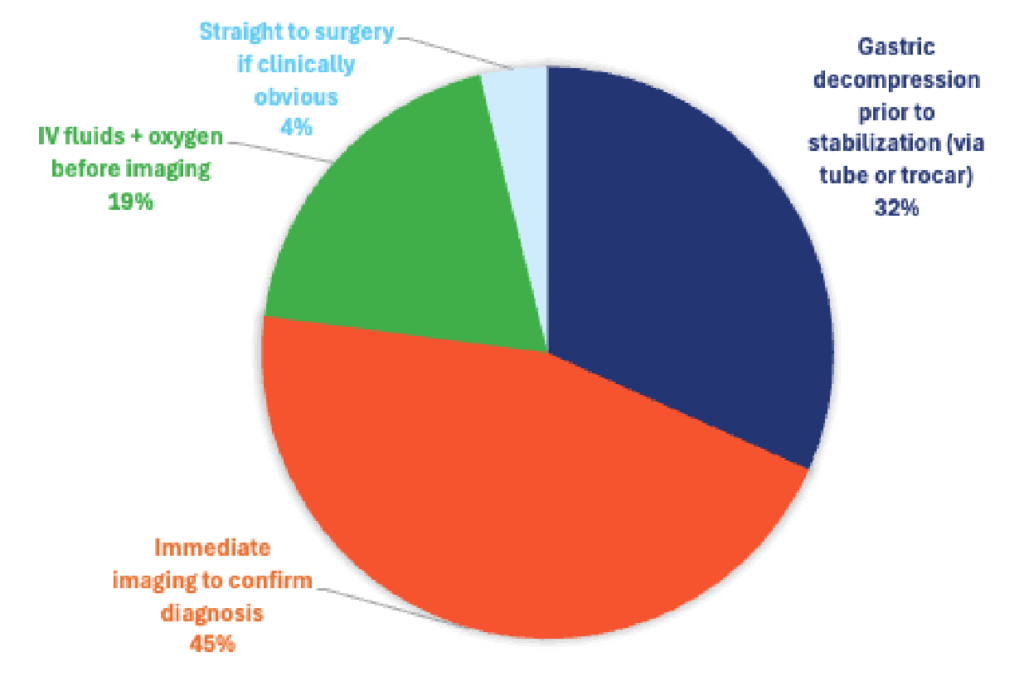
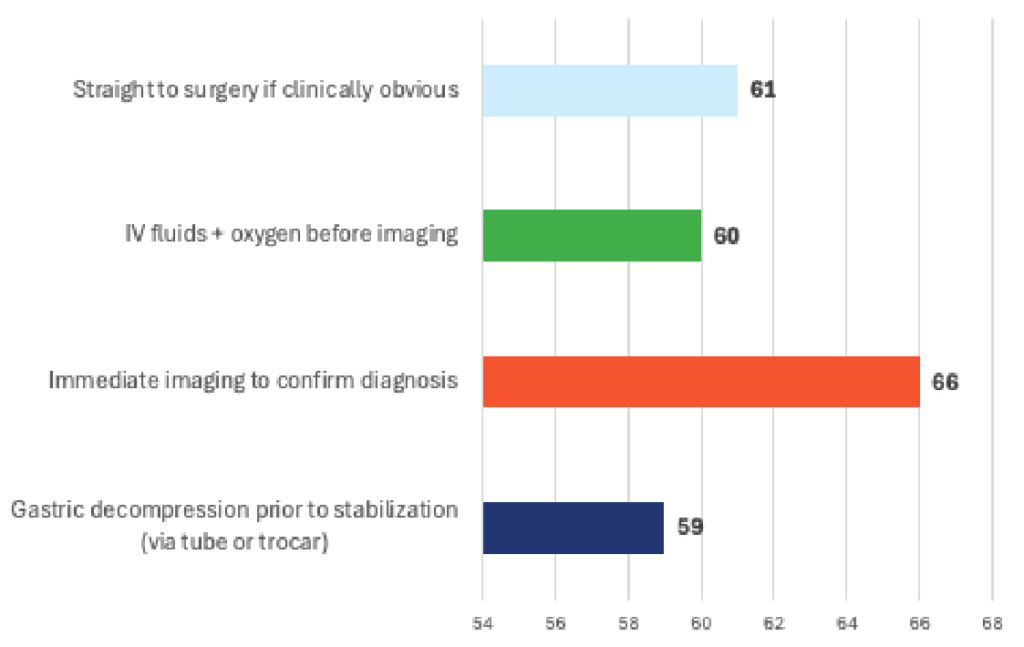
Effectiveness
Specialists Insight
IV Fluids + Oxygen Prior to Imaging
Purpose: Treat hypovolemic/obstructive shock, improve perfusion, stabilize cardiovascular status before anesthesia.
- GDV causes venous obstruction, reducing venous return and cardiac output → leads to shock.
- Immediate IV crystalloids (shock doses titrated to response) improve perfusion, cardiovascular stability, and reduce risk of anesthetic complications.
- Oxygen therapy improves hemoglobin saturation and supports perfusion until circulation returns.
Evidence on Outcomes
- Multiple retrospective studies (Fossum; Greenfield; Brockman et al.) consistently show improved survival when patients receive aggressive early fluid resuscitation.
- Stabilization reduces perianesthetic deaths, arrhythmias, and postoperative complications.
- Allows safe sedation/handling for decompression.
Effectiveness: High. Essential first step in most GDV protocols; directly improves survival.
Immediate Imaging to Confirm Diagnosis (e.g., Right Lateral Radiograph)
Purpose: Confirm volvulus and determine surgical urgency.
- The “double bubble” sign on right lateral radiograph is highly diagnostic.
- Imaging differentiates GDV from simple gastric dilatation or other abdominal processes.
Clinical Considerations
- Radiographs should not delay stabilization.
- In most cases, the patient is unstable; radiography while in shock is stressful and may worsen perfusion.
- A dog with classic signs (distention, unproductive retching, shock) often does not require imaging before emergency stabilization.
Effect on Outcomes
- Imaging is diagnostically valuable, but no evidence shows that radiographs improve survival if performed before stabilization.
- Conversely, delays in stabilization worsen outcomes.
Effectiveness: Moderate but not lifesaving. Necessary for confirmation prior to surgery, but should follow initial stabilization.
Gastric Decompression Prior to Full Stabilization (Orogastric Tube or Trocarization)
Purpose: Relieve gastric pressure, improve venous return, enhance ventilation, and reduce risk of gastric necrosis.
- Stomach distention causes caudal vena cava compression, which drives shock.
- Decompression immediately reduces pressure, often improving:
- Heart rate
- Blood pressure
- Lactate levels
- Respiratory effort
Tube vs. Trocar
- Orogastric tube: preferred when possible; confirms diagnosis and relieves large volumes of gas.
- Trocarization: faster and very effective when the patient is too unstable for tubing or tubing fails.
Evidence on Outcomes
- Early decompression (even before complete stabilization) is associated with:
- Lower lactate levels (a major prognostic factor)
- Improved hemodynamic parameters
- Reduced gastric necrosis
- Higher survival (Brourman et al., Brockman, Zacher et al.)
Many emergency specialists categorize decompression as part of initial stabilization, not something that waits for radiographs or full shock correction.
Effectiveness: Very High. One of the most impactful early interventions alongside fluids.
Straight to Surgery Without Stabilization (If Clinically Obvious)
Purpose: Avoid delays in correcting volvulus.
- The stomach is twisted → only surgical correction can resolve the volvulus.
- The argument for immediate surgery: “fix the problem now.”
Clinical Reality
- Most GDV patients are in hypovolemic shock; anesthesia induction in an unstable patient significantly increases perioperative mortality.
- Without stabilization:
- Arrhythmias increase
- Surgical mortality increases
- Risk of cardiac arrest increases
Evidence on Outcomes
- Multiple studies show that lack of preoperative stabilization is strongly associated with higher mortality.
- Dogs transported directly to surgery without fluids have markedly lower survival, especially if lactate is elevated.
Effectiveness: Low to Moderate. Only appropriate in extremely rare, highly controlled cases (e.g., already stabilized by referring vet). Generally contraindicated.
Most Effective First-Line Approach
Aggressive IV fluid resuscitation + oxygen IMMEDIATELY, followed by rapid gastric decompression (orogastric tube or trocar), before imaging or surgery.
This approach:
- Addresses shock, the major driver of mortality
- Reduces stomach pressure to restore venous return
- Lowers lactate (strong survival predictor)
- Creates a safer window for anesthesia and abdominal surgery
Imaging should occur only after initial stabilization and decompression, unless the diagnosis is uncertain. Surgery proceeds once the patient is hemodynamically improved.
Final Clinical Recommendation
The highest-survival protocol for suspected GDV is:
- Immediate IV fluids + oxygen
- Gastric decompression ASAP (tube or trocar—whichever is faster)
- Confirmatory radiographs once stable enough
- Proceed to surgery promptly after stabilization
This sequence is strongly associated with the best clinical outcomes and is widely supported in emergency and critical care literature