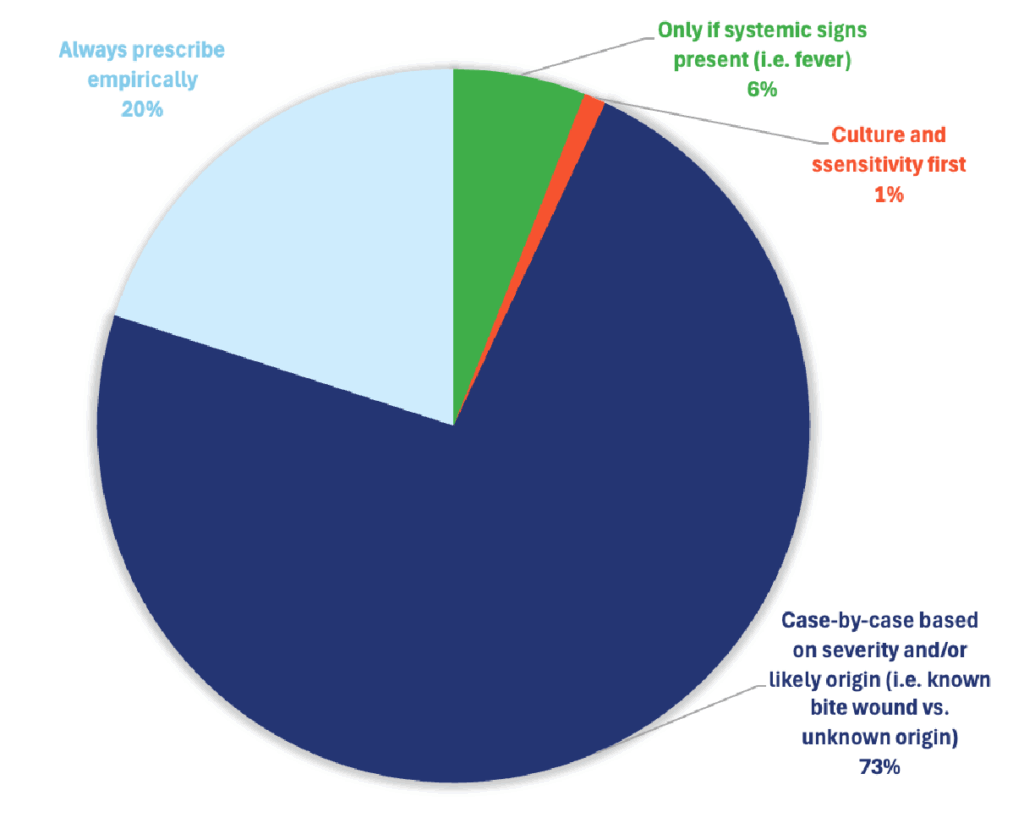
Responding DVMs overwhelmingly reported using a case-by-case clinical assessment when determining whether to initiate antibiotic therapy for localized wounds.

Localized Wound Care
Treatment Selections
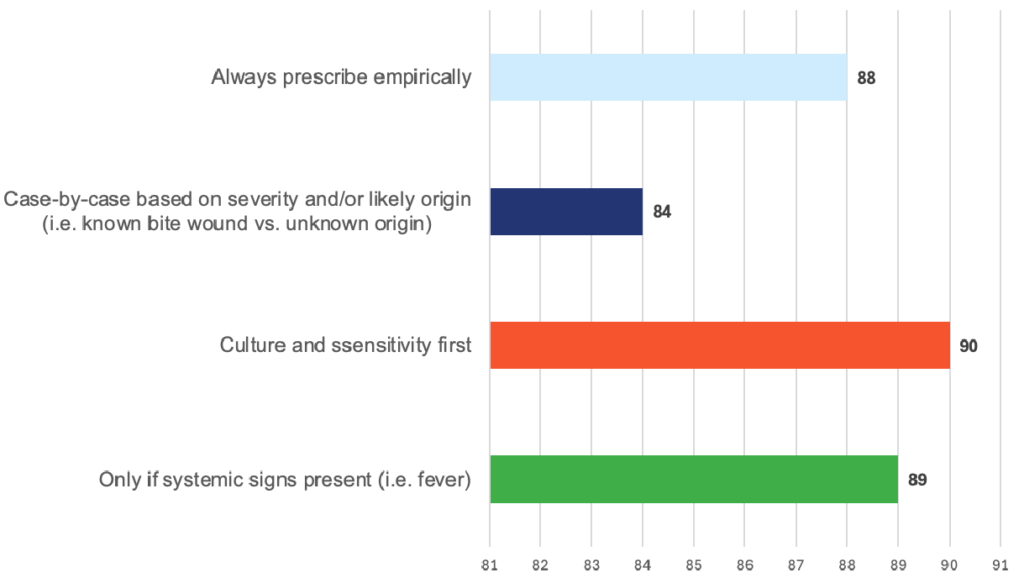
Effectiveness
Specialists Insight
For most localized skin wounds, specialists avoid routine antibiotics and instead focus on wound assessment, debridement, lavage, and drainage. Antibiotics are used only when indicated, and empirical use is not the default.
A. Always prescribe empirically
Estimated specialist responses: ~0–5%
Why so low:
- Specialist guidelines strongly discourage routine antibiotic use for superficial or uncomplicated wounds.
- Overuse drives antimicrobial resistance.
- Most localized wounds can be managed by local therapy alone.
Only a very small subset might say “always” for very specific wound types (e.g., typical cat bite abscess), but even then, they often consider it part of case-by-casedecision-making.
B. Culture and sensitivity first
Estimated specialist responses: ~10–20%
Interpretation: This means: “I rely on a culture before starting antibiotics for most cases.”
Why not higher:
- Culture and sensitivity is useful, but not required for every localized wound.
- Cultures are preferred for:
- Chronic, non-healing wounds
- Post-operative infections Suspicion of resistant organisms
- Deep tissue infections
- Not cost-effective or necessary for simple acute wounds.
Specialists often culture selectively, not universally.
C. Only if systemic signs (fever, etc.) present
Estimated specialist responses: ~15–25%
Why:
- Systemic illness increases the likelihood of invasive infection.
- Many specialists view systemic signs as a clear indication for antibiotics.
- However, absence of systemic signs does not rule out the need for antibiotics (e.g., cat bite abscesses may be localized but require treatment).
Specialists won’t limit antibiotic decisions only to systemic signs.
D. Case-by-case basis based on severity and likely origin
Estimated specialist responses: ~50–70% (most common response)
Why this is the top choice:
Specialists integrate factors such as:
- Wound origin:
- Cat bite abscess → antibiotics commonly indicated
- Shearing injuries → usually no antibiotics unless contamination or depth
- Surgical dehiscence → culture + targeted antibiotics
- Depth and contamination level
- Presence of abscess, cellulitis, purulence
- Patient factors:
- Immunocompromised
- Diabetic
- Geriatric
- On steroids
This answer aligns best with current ISCAID antimicrobial stewardship guidance and actual specialist behavior.
Most veterinary specialists choose Option D – they assess each wound individually, factoring in severity, contamination, likelihood of infection, patient risk factors, and whether the wound type (e.g., cat bite abscess) typically warrants antibiotics.