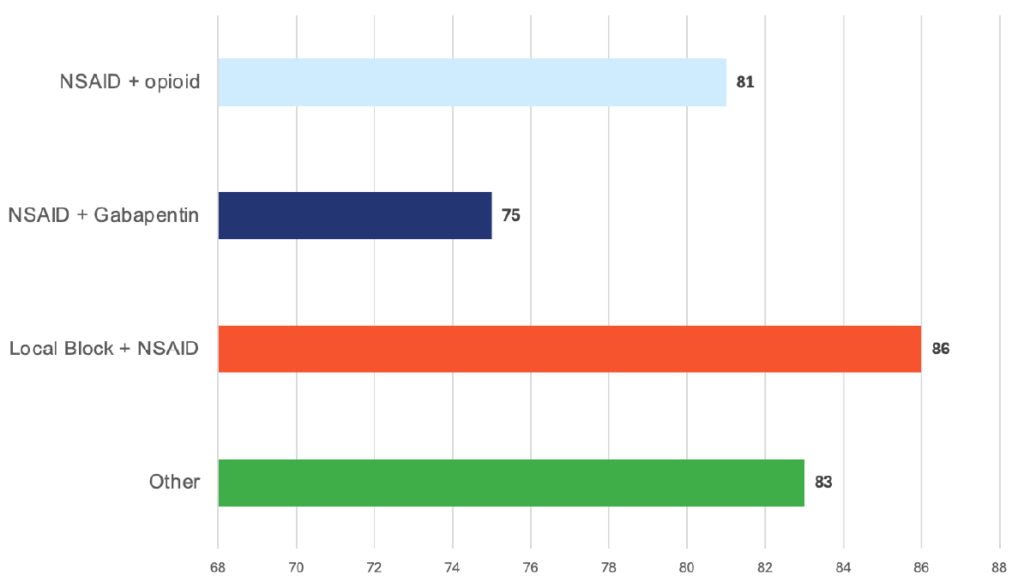
Responding DVMs elected NSAID + Gabapentin as their primary choice for postoperative pain in canines, while a close second was NSAID + opioid depending on the case.

Postoperative Pain
Treatment Selections

Effectiveness
Specialists Insight
For canine orthopedic surgery, the most reliable way to achieve consistent postoperative comfort is to treat pain from multiple angles— inflammation, nociception, and surgical-site transmission—rather than relying on a single drug class.
Why this approach works best
Contemporary pain management guidelines emphasize planning every orthopedic surgery around a multimodal framework, specifically:
- Opioid
- NSAID
- Local anesthetic technique
Local anesthetics are consistently highlighted as the most effective analgesic tools in small animal practice and should be incorporated into every orthopedic procedure, whenever feasible. Nonpharmacologic nursing measures (e.g., cold therapy, attentive postoperative care) further improve outcomes.
What Specialists Typically Do in Practice
For stifle and hip procedures, most specialists use:
- Ultrasound-guided femoral and sciatic nerve blocks or an epidural
- Systemic NSAID (if not contraindicated)
- Full μ-opioid in the immediate perioperative period
Randomized clinical studies show that femoral–sciatic nerve blocks provide analgesia comparable to epidural anesthesia for hind-limb orthopedic surgery, supporting either approach when properly performed.
Where Common Adjuncts Fit (and Don’t)
Gabapentin
- Not first-line for acute postoperative orthopedic pain in dogs
- In a randomized TPLO study, adding gabapentin (20 mg/kg q8h) to carprofen did not improve pain scores or limb function
- Rescue analgesia use was low and similar between groups
- Current guidelines place gabapentin (and tramadol) as lower-tier or adjunctive options, not core analgesics
Ketamine CRI
- Useful in select high-pain cases (e.g., amputations)
- Low-dose ketamine CRI can reduce central sensitization and opioid requirements
- Supported by clinical evidence showing improved postoperative comfort in dogs undergoing more painful procedures
A Practical “Default” Protocol for Typical Ortho Cases
Premedication: Opioid
→ Locoregional block: Femoral/sciatic block or epidural
→ Intraoperative: Opioid ± ketamine CRI (case-dependent)
→ Postoperative: NSAID + opioid as needed
→ Supportive care: Cold therapy and diligent nursing
How Often Does this Approach Produce Positive Cutcomes?
If “positive” is defined as good to excellent pai n control with minimal rescue analgesia and smooth recovery in the first 24–48 hours:
- Multimodal protocols incorporating locoregional anesthesia achieve effective analgesia in the majority of dogs (≈80–90%)
- Rescue analgesia rates are relatively low, often ≤20–30% in the first 24 hours, depending on procedure and assessment method
- Studies comparing femoral–sciatic blocks vs epidurals report similar pain scores and rescue requirements
- Adding gabapentin to NSAID-based protocols does not increase success rates in routine orthopedic cases
- In high-pain surgeries, adding a ketamine CRI can further improve comfort and increase the likelihood of a positive outcome
Bottom Line (Clinician Take-Home)
The most consistently effective, evidence-supported strategy for canineorthopedic postoperative pain is:
- NSAID + opioid + locoregional anesthesia, tailored to the individual patient.
- Adjuncts (ketamine CRI, alpha-2 agonists, lidocaine CRI in select scenarios) can belayered in for higher-pain cases.
- Routine gabapentin use for acute orthopedicpostoperative pain has not demonstrated benefit in dogs and should not replacecore analgesic strategies.