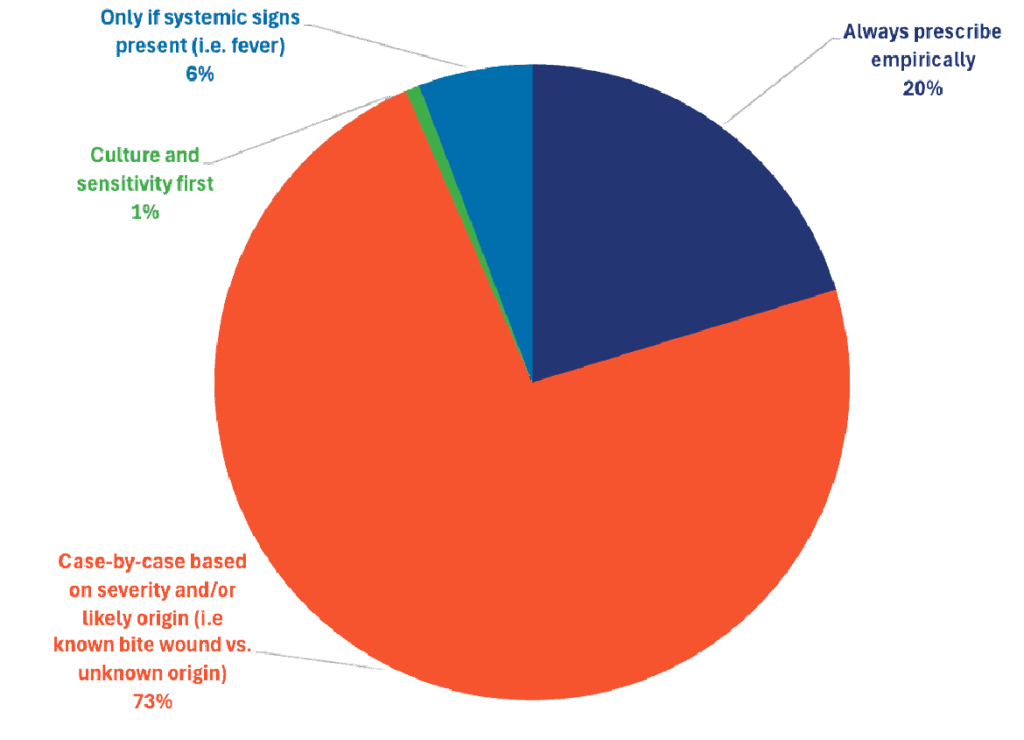
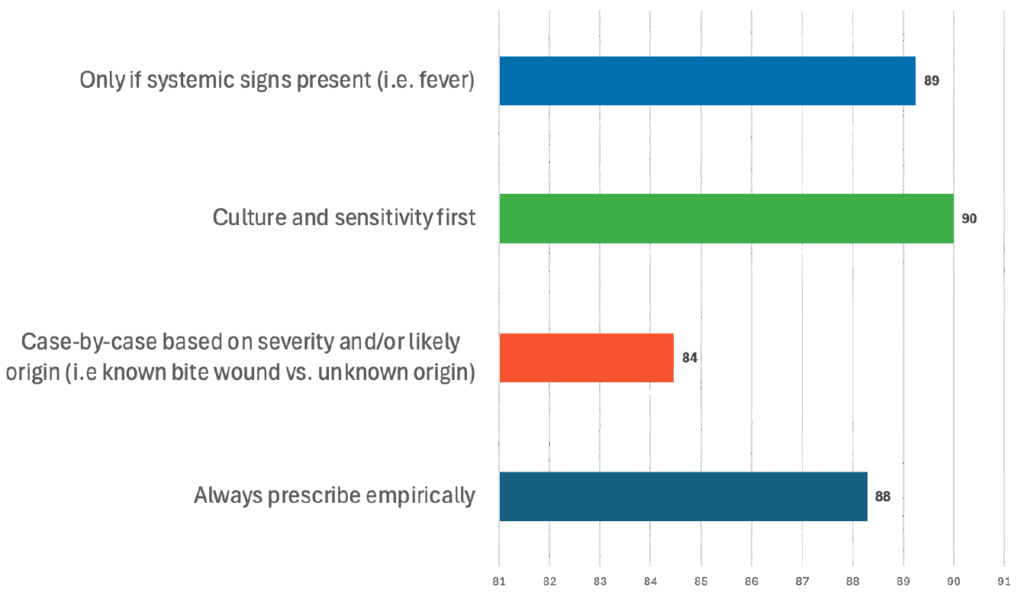
When asked how they approach surgical site infections, most responding DVMs described starting with the individual patient—73% said they make the diagnosis on a case-by-case basis. Even so, many pointed to what they feel works best in practice: empiric prescribing, which the majority believes leads to the strongest outcomes.

Surgical Site Infections in Canines
Treatment Selections
Effectiveness
Specialists Insight
Many specialists favor a beta‑lactam antibiotic active against skin flora (especially Staphylococcus pseudintermedius), typically either:
- Amoxicillin‑clavulanate (e.g., Clavamox) or
- A first‑generation cephalosporin (e.g., cephalexin, cefpodoxime).
- The logic: these cover the common skin pathogens; they are licensed, familiar, and typically effective in uncomplicated SSIs.
Treatment Effectiveness
While there is not a definitive percentage, many would estimate > 80% success in straightforward clean/clean‑contaminated SSIs when using appropriate antibiotic therapy plus surgical/wound management (debridement, drainage, good hygiene, etc.). Complexity factors (implants, immunocompromise, multidrug resistance) lower the success rate.
Supporting Evidence from Peer-Reviewed Literature
In a retrospective Finnish study of clean orthopaedic and neurosurgeries in dogs, SSI rate was ≈6.3%. Prophylaxis (cefazolin) was given, and omission of antibiotics did not significantly increase SSI risk in this low‑risk clean setting.
- Implication: Even in clean surgery, SSI risk is modest, and antimicrobial choice/timing matters more than simply “any antibiotic”.
A recent open‑access study (“Surgical Antibiotic Prophylaxis in Small Animal Surgery: A Retrospective Outcome‑Based Study…”, Animals, 2025) found that in clean or clean‑contaminated procedures without implants, no significant difference in SSI rates was seen among different prophylactic protocols.
- Implication: For prophylaxis (rather than active treatment of SSI), the spectrum and timing matter; also emphasizes surgery + wound care importance.
The WSAVA guideline document “Surgical Antibiotic Prophylaxis in Dogs (2024)” points out that the most common organisms in dog skin flora are Staph. pseudintermedius and that first‑generation cephalosporins or amoxicillin‑clavulanate are recommended when prophylaxis is indicated.
- Implication: This supports the choice of amoxicillin/clavulanate or cephalexin/cefpodoxime as a logical empiric first‑line.
Specialist Rationale Summary
- Empirical therapy for an uncomplicated, typical SSI often uses broad‐spectrum but skin‑flora‐targeted beta‐lactams (amox/clav) or first‐gen cephs.
- Culture + sensitivity is ideal in complicated cases (implant, MDR, immunocompromised) — many specialists will say “culture first‑line for complicated SSIs”.
- Success rates in straightforward cases are high (>80%), but outcomes drop when complicating factors exist (implant, drain, immunosuppression, resistant bacteria).
- Timing/prophylaxis (in the surgical setting) is less about long‑post‑op therapy, and more about peri‐operative antibiotic at correct timing plus asepsis.