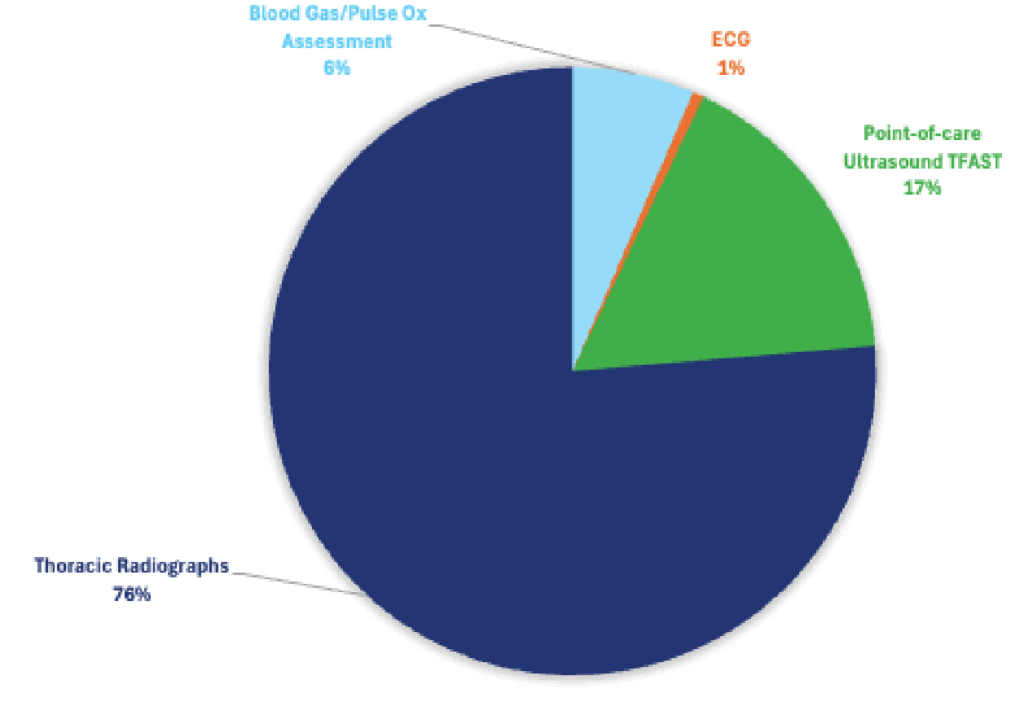
Among responding DVMs, thoracic radiographs were the primary treatment option for acute respiratory distress.

Acute Respiratory Distress
Treatment Selections
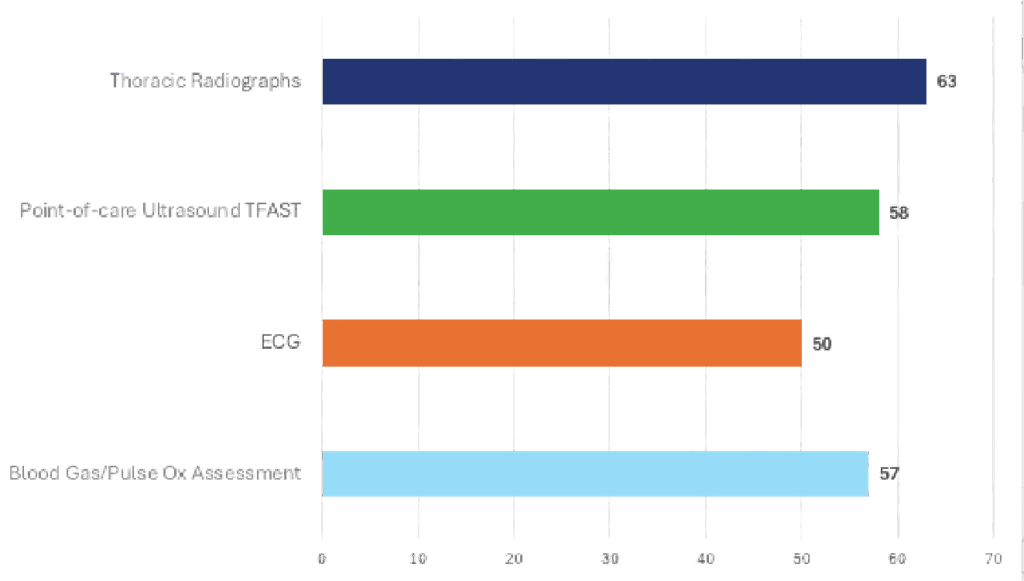
Effectiveness of Treatment
Specialists Insight
Why Specialists Choose TFAST First
In an acutely dyspneic patient, specialists prioritize diagnostics that are:
- Rapid
- Minimally stressful
- Performable while the patient remains in oxygen
- Possible without repositioning
Key Advantages of TFAST
- Completed in < 2–3 minutes
- No lateral or DV positioning required
- Rapidly identifies immediately lifethreatening conditions, including:
- Pleural effusion
- Pneumothorax
- Pericardial effusion
- Pulmonary edema (B-lines)
- Directly guides immediate interventions, such as:
- Thoracocentesis
- Pericardiocentesis
- Lower risk of decompensation compared with radiographs in unstable patients
As a result, specialists generally delay thoracic radiographs until the patient is stabilized or a reversible cause is identified via TFAST.
How Specialists Rank the Options
- Point-of-care ultrasound (TFAST)
- Blood gas / pulse oximetry (adjunctive, not primary)
- Thoracic radiographs (after stabilization)
- ECG (rarely helpful for primary respiratory distress)
Approximately 80–95% of cases show clinical benefit from early TFAST use.
What “Positive Outcome” Means to Specialists
- Faster identification of the cause of dyspnea
- Earlier, targeted intervention
- Reduced patient stress and hypoxemia
- Decreased morbidity and mortality
- Fewer delays to lifesaving procedures
Supporting Evidence
- TFAST demonstrates high sensitivity and specificity for:
- Pleural effusion
- Pneumothorax
- Pericardial effusion
- Early ultrasound-guided intervention is associated with:
- Shorter time to diagnosis
- Reduced reliance on emergency radiographs
- Improved stabilization success
In practice, specialists report that TFAST changes case management in the majority of dyspneic patients, often within minutes of arrival.