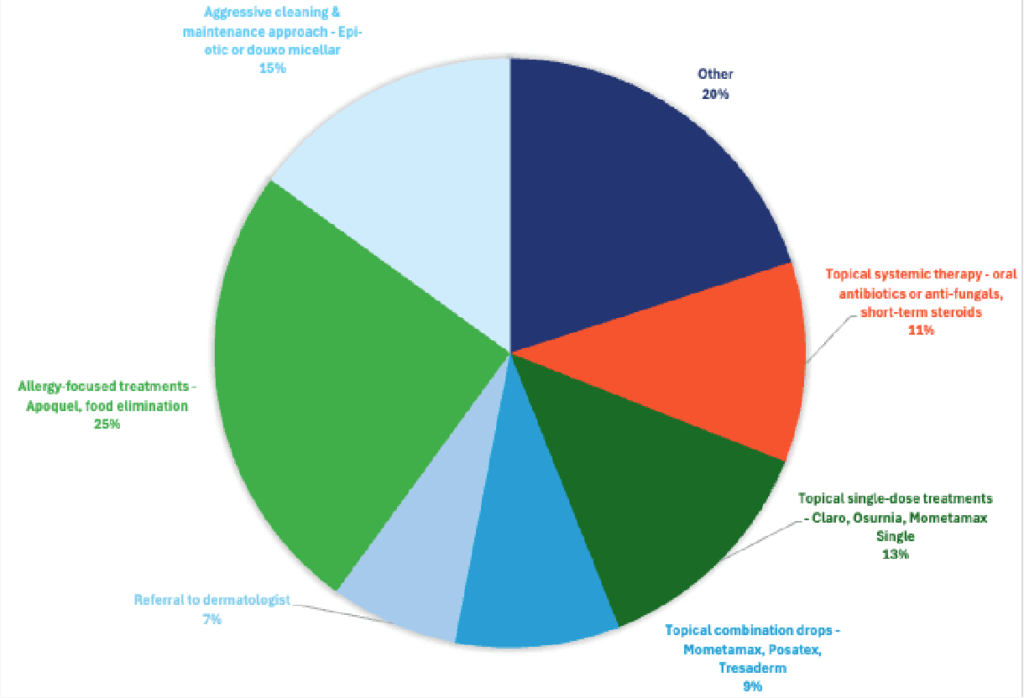
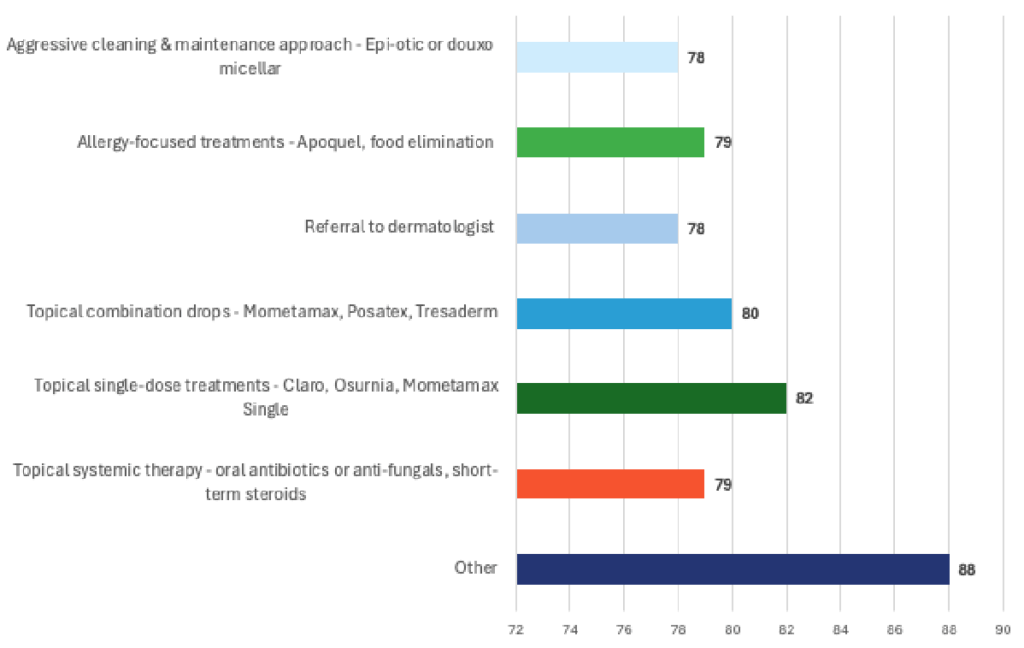
Responding DVMs most often reported choosing an allergy-focused approach as their primary strategy for managing chronic ear infections, while the majority said the best outcomes typically come from combining multiple therapies.

Chronic Ear Infections
Treatment Selections
Effectiveness
Specialists Insight
Topical combination drops remain the first-line “go-to” for most specialists, but always within a multimodal framework that includes:
- Cytology guided treatment
- Ear cleaning and maintenance,
- Identification and management of underlying causes (especially allergies), and
- Judicious use of systemic or singledose formulations in select cases.
Treatment Options
Topical combination drops (Mometamax, Posatex, Tresaderm, etc.)
- Strengths: These offer targeted antimicrobial + antifungal + anti-inflammatory effects locally with relatively high concentrations and minimal systemic side effects. They are a cornerstone in induction therapy of flares.
- Limitations: They must be matched to the cytologic findings or culture results, used in sufficient volume, and for a long enough duration— often extending beyond clinical resolution. Repeated use can drive resistance if not used judiciously.
- In recurrent/chronic cases, the specialist uses these drops in the flare-control “induction” phase.
Aggressive cleaning & maintenance approach (Epi-otic, Douxo micellar, etc.)
- Strengths: Essential adjunct. Removing debris, exudate, biofilm, and wax improves penetration of topicals and reduces microbial load. A “clean ear” is a prerequisite to successful therapy.
- Limitations: Overzealous or overly frequent cleaning can injure delicate tissues; in ears with ruptured tympanic membranes, some agents risk ototoxicity. But as part of a maintenance plan, it is indispensable.
Topical single-dose treatments (Claro, Osurnia, Mometamax Single, etc.)
- Strengths: Convenient (less frequent dosing) which may improve compliance. Useful in mild to moderate cases where cytology is clear and the pathogen is susceptible.
- Limitations: In more complicated or chronic ears with dense exudate, hyperplasia, stenosis, or biofilm, a single or infrequent dose may not be adequate to penetrate and fully suppress the infection. Furthermore, during therapy, cleaning is typically limited.
Allergy-focused treatments (Apoquel, food elimination, immunotherapy, etc.)
- Strengths: Many chronic otitis cases are secondary to allergies (atopic dermatitis, food hypersensitivity). Addressing the allergic driver is vital to reducing recurrence.
- Limitations: These therapies take time (weeks to months) to show effect. They seldom are suffice alone when an active infection is present. They are part of the maintenance / preventative strategy, not the acute flare control.
Topical single-dose treatments (Claro, Osurnia, Mometamax Single, etc.)
- Strengths: Systemic therapy is often indicated in more severe, proliferative, chronic, or middle ear–involved cases, or when topical access is difficult. Steroids help reduce inflammation and canal narrowing.
- Limitations: Risks of systemic side effects, antimicrobial resistance, cost, and systemic immunosuppression. Must be used judiciously and ideally guided by culture/sensitivity if rods or difficult organisms are involved.
Referral to dermatologist
- Strengths: Ear specialists/dermatologists bring advanced diagnostics (videootoscopy, CT imaging, biopsies, allergen testing) and may consider surgical salvage earlier. Complex or refractory cases benefit from referral sooner rather than later.
- Limitations: Access, cost, and geographic considerations may limit referral for many clients. But it should not be delayed in cases not responding to appropriate therapy.
Specialist’s Ideal Protocol
1. Comprehensive diagnostics
- Otoscopic exam, cytology (bacteria + yeast), culture & sensitivity when indicated (especially for rods or non-responders).
- Evaluate and test for underlying etiologies: allergies (food trial, intradermal/serum testing), endocrinopathies, anatomical conformation, foreign bodies, etc.
- Imaging and middle ear assessment if otitis media/interna suspected.
2. Ear cleaning / debridement (“reset the terrain”)
- In the clinic under sedation or anesthesia if needed, flush and remove debris, exudate, biofilm, wax. Use non-irritating cleansers approved for ears, mindful of tympanic membrane integrity.
- Post-cleaning, dry the canal and ensure it’s as clean as possible before applying medicated therapy.
3. Induction therapy to achieve remission
- Apply topical combination drops (antibiotic + antifungal + steroid) tailored to cytology/culture. Use adequate volume to fill the canal and massage to distribute.
- Concurrent topical steroids (in the combination) help reduce inflammation, canal narrowing, and facilitate healing.
- Use of systemic therapy only when necessary (severe, proliferative disease, suspected otitis media, deep tissue involvement) under guidance of culture/antibiogram.
- In mild to moderate cases with known susceptible organisms, topical singledose products (Claro, Osurnia, Mometamax Single) may be used, though more cautiously in recurrent/chronic ears.
4. Maintenance / prevention of relapse
- Scheduled ear cleaning / drying / use of antiseptic/drying agents (e.g., micellar ear cleaners, Epi-otic, drying solutions) to maintain a “low microbial load” environment.
- Low-potency topical steroids or intermittent anti-inflammatory therapy to control residual irritation.
- Allergy management becomes central: food trials, allergen immunotherapy, strict flea prevention—these reduce the driver of inflammation.
- Frequent rechecks with cytology to catch relapses early.
5. Consider referral / surgery when needed
- If medical therapy fails repeatedly, structural damage is advanced (fibrosis, stenosis, ossification), or middle ear disease is present, referral to a veterinary dermatologist or surgeon is appropriate. In extreme cases, total ear canal ablation + lateral bulla osteotomy (TECA/LBO) may be curative but comes with significant morbidity.
| Tier | Strategy | Goal |
|---|---|---|
| 1. Single-dose topicals (Claro®, Osurnia®, Mometamax Single) | Simplify care & improve compliance | Short-term infection resolution |
| 2. Topical combo drops | Gold standard for chronic cases | Cytology-guided infection control |
| 3. Systemic + Topical + Anti-inflammatory | For severe/chronic infections | Deep tissue resolution |
| 4. Maintenance + Allergy mgmt. | Prevent relapse | Long-term stability |
| 5. Referral / Surgery | Salvage option | Comfort & cure in endstage ears |
Did You Know?
Many “recurrent otitis externa” cases actually have otitis media underlying it, so dogs relapse quickly and it can look like “resistance.” In those cases, the middle ear acts like a reservoir, and outcomes often improve only after deeper evaluation (e.g., sedated otoscopy/videootoscopy ± imaging) and a different plan.
Specialist Flowchart: Managing Chronic & Recurrent Canine Otitis Externa
| Phase | Goal | Key Steps (Bullets) | When to Culture/Refer | Home Care/Notes | Escalation Trigger |
|---|---|---|---|---|---|
| 1) Diagnostic & Assessment | Identify cause → classify severity → guide targeted therapy. | • Cytology: cocci, rods, or yeast? • Otoscopy ± sedation • Evaluate underlying causes: allergy, endocrine disease, anatomy |
• Culture if rods or refractory • Early derm referral if otitis media suspected or proliferative change |
- | Suspect otitis media / proliferative change |
| 2) Cleaning & Debridement | Clear debris, wax, and biofilm for drug penetration. | • In-clinic ear flush: TrizEDTA, saline, micellar cleansers • Avoid ototoxic agents if TM compromised |
- | • Home maintenance: Epi-Otic / Douxo Micellar • “Clean ear = Treatable ear!” |
TM compromised / pain limits exam |
| 3) Induction / Infection Control | Control infection based on severity & cytology/culture. | • Choose topical/single-dose vs combo drops vs systemic plan | • Culture guided therapy for rods, chronic/refractory cases | • Recheck cytology in 2–3 weeks for uncomplicated cases | Rods, stenosis, ulceration, severe pain |
| 4) Inflammation & Pain Control | Open canal, improve airflow, enhance drug absorption. | • Topical steroid (combo products) • Short course oral pred / Apoquel / Cytopoint as appropriate |
- | - | Marked edema/stenosis ; ongoing pain/itch |
| 5) Maintenance & Recurrence Prevention | Prevent relapse; manage underlying drivers long-term. | • Topical steroid (combo products) • Short course oral pred / Apoquel / Cytopoint as appropriate |
- | • Manage allergies: Apoquel, Cytopoint, immunotherapy • Food trial if suspected • Reduce humidity/water exposure |
≥3 infections/year despite maintenance |
| 6) Referral / Surgical Tier | Escalate for advanced diagnostics/ procedures/end-stage disease. | • Dermatology referral criteria: – 3 infections/year – Canal stenosis/ mineralization – Failure despite culture-guided therapy | - | • Advanced options: video otoscopy, laser canal plasty • TECA/LBO for end-stage disease |
End-stage, mineralized/stenotic canal; chronic otitis media |