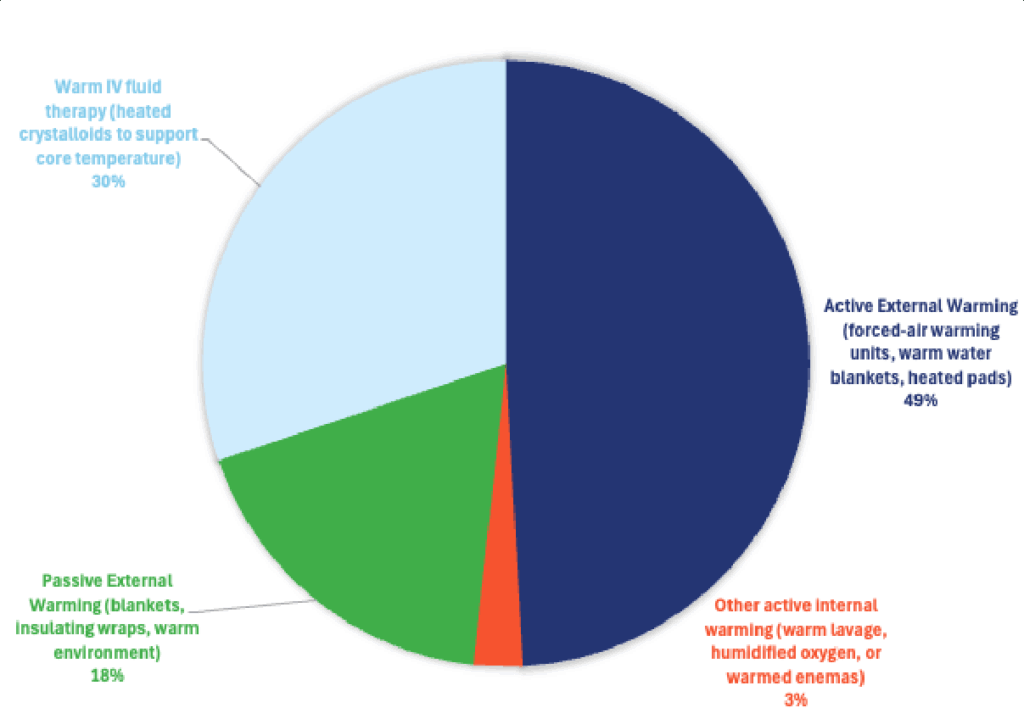
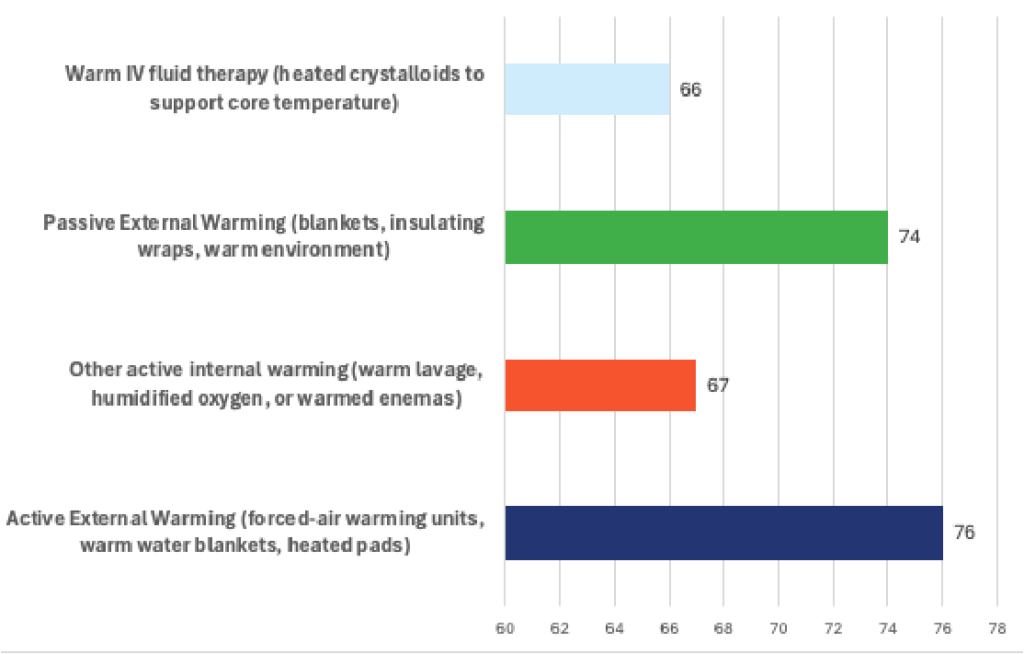
Among responding DVMs, active external warming—including forced-air warming systems, warm water blankets, and regulated heating pads—was the most frequently selected initial intervention for canine hypothermia. Clinicians who reported using active external warming cited an average effectiveness of 76% in achieving clinically meaningful improvement in patient temperature and stability. This preference likely reflects the modality’s broad availability, rapid heat delivery, and ease of integration with supportive therapies, particularly warmed IV fluid administration and passive insulation. While respondents recognized the need for careful monitoring to avoid peripheral vasodilation and hypotension, active external warming was consistently viewed as a practical and effective first-line component of multimodal rewarming protocols in hypothermic canine patients.

Hypothermia
Specialists Insight
“In hypothermic dogs, the most effective prevention of rebound hypothermia and shock is achieved through a controlled, multimodal approach combining passive insulation, active external warming, and warmed intravenous fluids, with active internal rewarming reserved for severe or refractory cases.”
Active External Warming
Commonly selected and strongly supported, especially for mild–moderate hypothermia.
- Forced-air warming systems (e.g., Bair Hugger–type devices)
- Circulating warm-water blankets
- Heated pads (with strict temperature monitoring)
Rationale: Active external warming is effective at increasing peripheral and core temperature when combined with careful monitoring. Forced-air systems provide uniform heat distribution and reduce the risk of focal thermal injury. Specialists emphasize gradual rewarming to avoid peripheral vasodilation–induced hypotension.
Passive External Warming
Almost universally selected as a baseline intervention.
- Dry blankets
- Insulating wraps
- Warm, draft-free environment
Rationale: Passive warming is essential to prevent further heat loss and is appropriate for mild hypothermia or as an adjunct in moderate to severe cases. It reduces metabolic demand and minimizes the risk of rebound hypothermia when combined with active methods.
Warm IV Fluid Therapy
Frequently selected as an adjunct, not as a sole method.
- Crystalloids warmed to ~38–40°C (100–104°F)
Rationale: Warm IV fluids help prevent iatrogenic heat loss and support perfusion, but do not significantly raise core temperature alone. Specialists stress that unwarmed fluids can worsen hypothermia and contribute to shock.
Other Active Internal Warming (Case-dependent)
Selected selectively, usually for moderate–severe hypothermia or refractory cases.
- Warmed body cavity lavage (gastric, bladder, peritoneal, thoracic)
- Heated, humidified oxygen
- Warm enemas (used cautiously)
Rationale: Internal rewarming techniques increase core temperature more directly but carry greater risk (arrhythmias, fluid shifts, infection). These methods are generally reserved for critical patients, often under anesthesia or intensive care.
Key specialist consensus points
- Multimodal rewarming is most effective (passive + active external ± warmed fluids).
- Gradual rewarming (≈0.5–1.0°C/hour) reduces the risk of:
- Rebound hypothermia
- Hypotension
- Ventricular arrhythmias
- Continuous temperature, blood pressure, and ECG monitoring is essential.
- Overly aggressive peripheral warming without volume support increases shock risk.