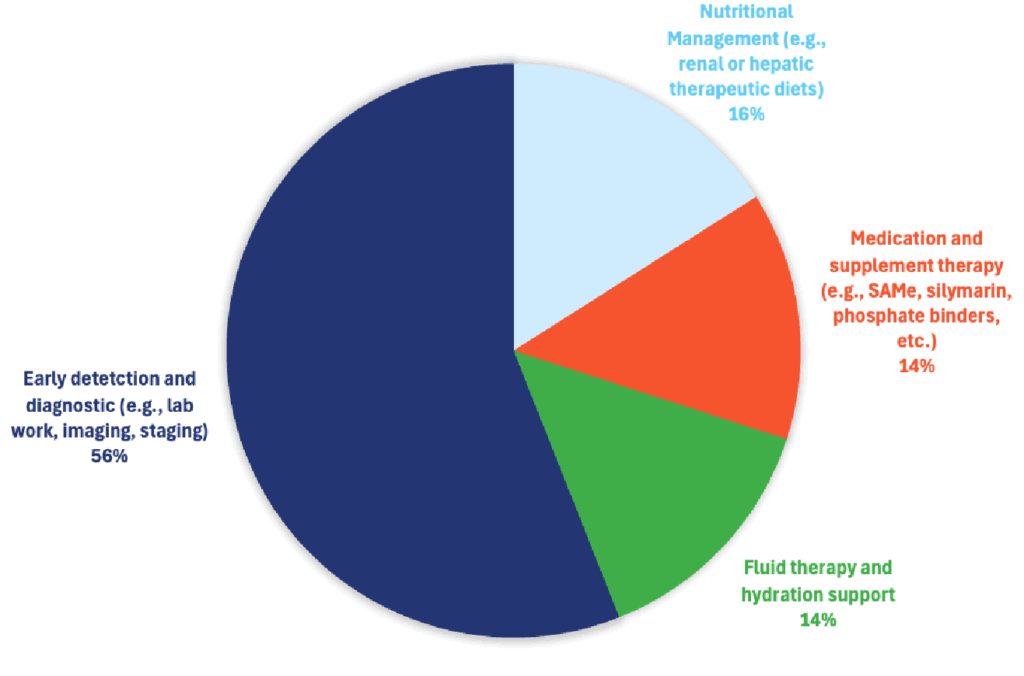
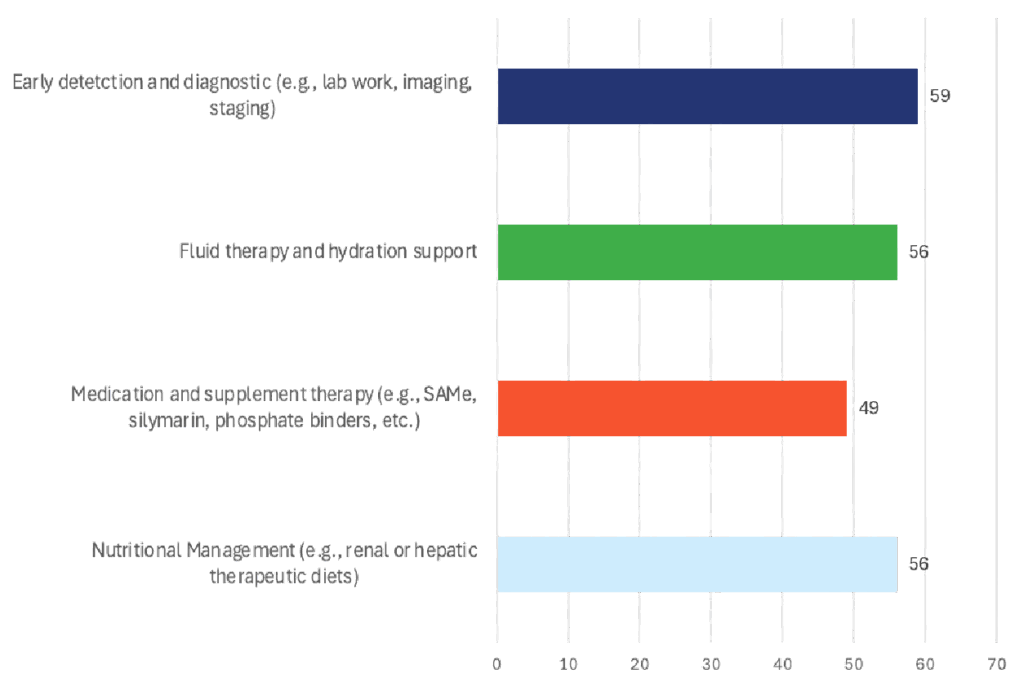
56% of responding DVMs said that early detection and diagnostic workups enable more effective management of kidney and liver disease, with an estimated effectiveness of 59% across cases.

Kidney/Liver Disease
Treatment Selections
Effectiveness
Specialists Insight
Kidney disease – Chronic (CKD): Nutritional management — specifically a therapeutic renal diet (restricted phosphorus, adjusted high-quality protein, alkalinizing, omega-3s) has the strongest, repeated, survival benefit in both cats and dogs. Early detection and good diagnostics matter because they let you start the diet and control complications (proteinuria, hypertension) sooner, but the largest proven effect size on survival comes from the diet.
Kidney disease – Acute (AKI): Rapid hydration and fluid therapy (with careful monitoring to avoid fluid overload) plus addressing the inciting cause are the highest-impact acute interventions. Mortality in AKI is still high; best-practice guidelines emphasize prompt fluids but warn that fluid overload worsens outcomes.
Liver disease: The single “greatest” intervention depends on etiology. For chronic hepatitis (especially copper-associated), early diagnostic work-up (including biopsy and copper quantification) that enables targeted therapy (copper chelation and long-term copper-restricted nutrition ± zinc) is what most improves prognosis. Broad “liver supplements” have mixed evidence; targeted, etiology-driven care is key.
Improving Outcomes
Early detection & diagnostics
Why specialists value it: It unlocks the right treatment early (diet, antihypertensives/RAAS blockers, phosphate control for CKD; biopsy and copper quantification for hepatopathies; rapid AKI triage).
Outcome links:
- CKD: Early staging (IRIS) and work-ups (BP, UPC, phosphorus/FGF-23, SDMA/creatinine trends) guide timely renal diet and renoprotective therapy, which improves survival and slows complications.
- Liver: For dogs with suspected chronic hepatitis, ACVIM recommends diagnostic confirmation and etiologic classification (e.g., copper-associated) to enable diseasemodifying therapy — an approach associated with better long-term control than nonspecific “support.”
- AKI: New IRIS best-practice consensus (2024) stresses early recognition/grading and directed diagnostics to guide fluid therapy and cause-specific treatment; despite this, AKI mortality remains high, underscoring the need for swift action.
- When it’s “greatest”: Whenever a disease is treatable if found early — e.g., copperassociated hepatitis or proteinuric/hypertensive CKD — early detection is the essential first domino.
Nutritional Management
Why specialists prioritize it (CKD): Multiple prospective and retrospective clinical trials show renal diets prolong survival and reduce uremic crises in naturally occurring CKD.
Outcome data highlights:
- Cats with CKD: Median survival ~16–21 months on renal diets vs ~7–9 months on maintenance diets.
- Dogs with CKD: A blinded RCT showed fewer uremic crises and lower mortality versus maintenance food.
- Guidelines: IRIS treatment recommendations place renal diet at the center of CKD care to slow progression and manage mineral-bone disorder (e.g., via phosphorus/FGF-23 control).
- Liver disease: Diet becomes “greatest” when it is etiology-targeted (e.g., copperrestricted diets ± zinc for copper-associated hepatitis), which can reduce hepatic copper and improve clinical control.
Hydration & Fluid Therapy
Why specialists prioritize it (AKI): Restores perfusion, corrects dehydration, buys time for renal recovery and definitive care. But precise monitoring is critical; fluid overload worsens outcomes.
Outcome & guidance:
- AKI mortality remains ~45–60%, so early, carefully titrated fluids are pivotal; consensus guidelines emphasize avoiding positive fluid balance.
- CKD (decompensations): Short courses of IV fluids or at-home assisted hydration can relieve uremic signs, but they do not replace the long-term survival benefits of renal diets and proteinuria/BP control. (Guideline-based practice.)
- When it’s “greatest”: AKI and any hypovolemic/dehydrated patient — immediate life-saving impact.
Medication & Supplement Treatments
Kidney (CKD):
- RAAS blockers (ACEi/ARBs) reduce proteinuria (a negative prognostic factor) and are often used alongside diet; telmisartan is non-inferior to benazepril for lowering UPC in cats with CKD. Some canine trials suggest improved renalevent–free survival with benazepril.
- Phosphate binders, antihypertensives, antiemetics, appetite support: improve QOL and help meet diet targets; outcome data are supportive but generally less dramatic than diet.
Liver:
- Targeted therapy changes outcomes (e.g., d-penicillamine chelation and copper-restricted diet ± zinc for copper-associated hepatitis). ACVIM’s consensus emphasizes etiology-driven regimens; evidence for general hepatoprotectants (e.g., SAMe, silybin) is mixed and often biomarker-based rather than hard-outcome-based.
When it’s “greatest”:
- Proteinuric/hypertensive CKD (RAAS blockade alongside diet).
- Etiology-defined hepatopathies (e.g., copper-associated) where drugs/nutrition remove the cause of ongoing liver damage.
Overall Preference
If you must pick a single intervention with the largest proven impact on survival in routine practice: Nutritional management (renal diets) for CKD. The effect sizes in cats and dogs are larger and more consistent than for any other single measure.
For AKI, timely, carefully managed fluid therapy is the most impactful immediate intervention; it determines short-term survival while you pursue the cause.
For liver disease, the “greatest” intervention is early diagnostics that enable targeted therapy (e.g., copper quantification → chelation + copper-restricted diet). That disease-specific approach changes trajectory more than nonspecific supplements alone.
Quick Take For Your Team
If you’re choosing one lever to standardize across practices this week:
- Make sure every CKD patient is actually on a therapeutic renal diet (and eating it), with owner coaching and escalation (flavor trials, appetite support, feeding tubes when appropriate). That’s the highest, most consistent impact on survival we can deliver in general practice.
- In AKI, drill the triage → fluids (avoid overload) → cause-directed care reflex.
- For liver, invest in early, definitive diagnostics (including biopsy) to identify copper-associated disease and treat the cause (chelation + copper-restricted diet).
Practical care pathway specialists use (kidneys & liver)
- Screen & stage early (IRIS: chemistry, SDMA/creatinine trends, UA/UPC, BP; liver imaging, bile acids, and biopsy when indicated).
- Start the right diet early (renal diet for CKD; copper-restricted diet for copper hepatopathy).
- Stabilize perfusion & fluids (especially AKI; avoid overload).
- Add targeted meds (RAAS blockade for proteinuria/hypertension in CKD; chelation/ursodeoxycholic acid/immunosuppression only when indicated by diagnosis in hepatic disease).
- Monitor and iterate (phosphorus/FGF-23, BP, UPC; recheck liver enzymes and copper; adjust plan).