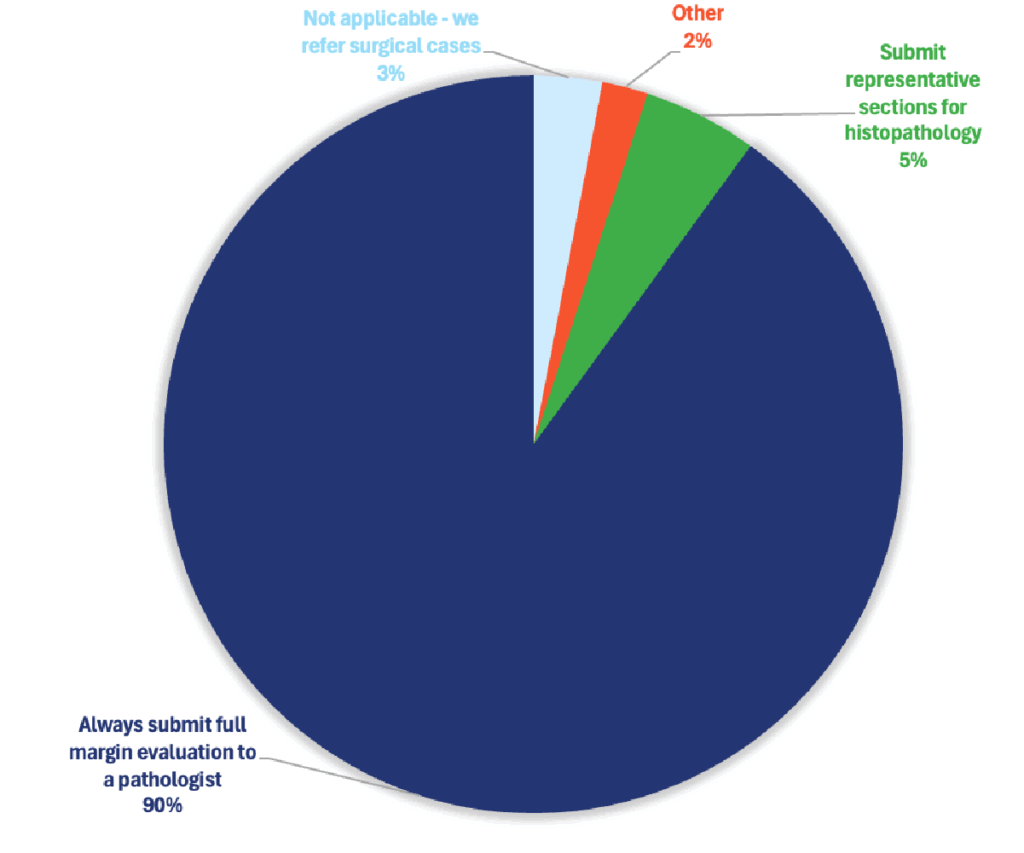
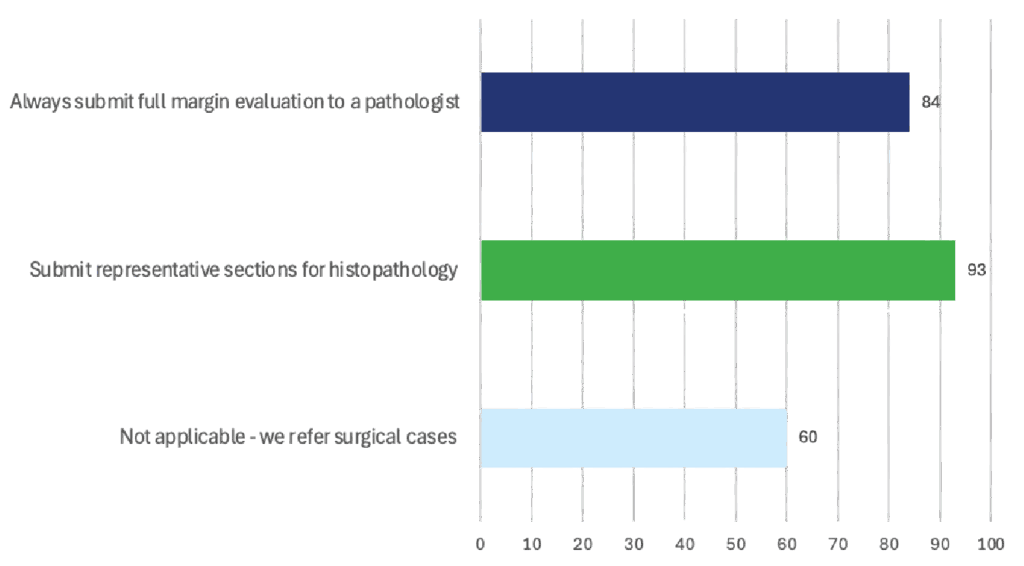
The majority of DVM respondents (90%) indicated that when performing malignant excisions, they routinely submit samples for full margin evaluation by a pathologist. This practice demonstrated an overall efficacy rating of 84%.

Malignant Tumor Excision
Treatment Selections
Effectiveness
Specialists Insight
In specialty oncology practice, surgical margins are almost always evaluated histologically using representative sectioning rather than full circumferential sampling. This approach yields histologically complete excision in roughly two-thirds of malignant tumor cases and results in durable local control in 80–90 % of those. Margin status remains one of the most powerful prognostic indicators for recurrence, but its predictive accuracy depends on tumor type, anatomic site, and completeness of sampling.
How Often Do We Get Clear Margins and Good Outcomes?
Even with great surgery and careful lab work, there are limits to what we can see under the microscope. Whether a tumor is truly “all gone” depends on many factors — the type of tumor, its grade (how aggressive it is), its location, how it grows, how the surgery is planned, and whether additional treatments (like radiation or chemo) are used.
Table: Margin Evaluation Methods, Expected Clear-Margin Rates, and Outcomes by Tumor Type
| Tumor Type | Typical Margin Evaluation Method (Specialist Practice) | Histologically “Clean” Margin Rate | Local Recurrence (Clean Margins) | Local Recurrence (Incomplete/Close Margins) | Key Notes / Specialist Perspective |
|---|---|---|---|---|---|
| Canine Cutaneous Mast Cell Tumor (MCT) | Representative sections (“breadloafing”); full margin on high-grade or recurrent cases | ~80–90 % (with ≥2 cm margins or proportional margins) | 5–10 % | 25–45 % | Margin width correlates with grade and recurrence. Specialists often use proportional margins (tumor diameter × 1) for low/intermediate grade. Adjuvant therapy considered for high-grade or narrow margins. |
| Canine Soft Tissue Sarcoma (STS) | Representative sections, often with inked margins and radial sectioning | ~55–75 % | 5–15 % | 30–50 % | Margins ≥3 cm laterally and one fascial plane deep recommended. Clean margins strongly reduce recurrence risk. Infiltrative STS and oral STS have higher recurrence despite clean margins. |
| Canine/Feline Carcinomas (cutaneous or subcutaneous) | Representative sections ± tangential en face on high-risk zones | ~50–70 % | 10–20 % | 35–60 % | Tumor type (SCC vs. adenocarcinoma) and anatomic site critical. Ear and nasal planum carcinomas often need adjunct therapy despite clean margins. |
| Feline Injection-Site Sarcoma (FISS) | Wide excision or referral to specialist center; complete margin mapping recommended | 40–60 % | 10–25 % | 50–70 % | High local recurrence risk; specialists usually refer to oncology centers for CT-guided wide excision (3–5 cm margins) or radiation adjunct. Full margin mapping ideal but costly. |
| Oral/Maxillofacial Tumors (MCT, SCC, Melanoma, Fibrosarcoma) | Representative sections + intraoperative imaging/guidance | 45–65 % | 10–25 % | 45–70 % | Complex anatomy makes full margins rare. Specialists rely on CT or MRI planning and sometimes intraoperative frozen sections. |
| Overall Across Malignant Tumors (specialist estimate) | Representative histologic margin assessment | 60–75 % | 5–15 % | 30–50 % | Clear histologic margins correlate with markedly better long-term local control and survival. “Clean” ≠ guarantee— sampling limitations exist. |
What the Research Shows
- In one study of 60 tumors, about half (48%) had completely clean margins, 18% were narrow, and 33% still had tumor cells at the edge.
- Tumors with clean margins recurred in only 10% of cases, but recurrence jumped to 70–80% when margins weren’t clean.
- For soft tissue sarcomas, clean margins lowered the chance of recurrence by about 60%.
- Another study found:
- 7% recurrence when margins were truly clean
- 23% when margins were “narrow”
- 42% when tumor cells were still present
- For mast cell tumors, when surgeons took about 2 cm of tissue around the tumor, they got complete removal in over 85% of cases, with very low recurrence in low-grade tumors.
What Specialists Say in Practice
- With careful planning and the right surgical margins, 50–80% of surgeries can achieve truly clean margins, especially for low-grade or well-defined tumors.
- For aggressive or hard-to-reach tumors, clean margins are harder to get, and recurrence is more likely—even if the lab report says “clean.”
- A “clean margin” greatly lowers the risk of regrowth, but it’s not a 100% guarantee. Sometimes a tumor comes back even when the report looks good, and sometimes “incomplete” removals never cause problems.
If you ask a specialist how often this method works, most would say:
In about 60–70% of cases, we get clean margins. Of those, 80–90% of pets stay tumor-free long-term, especially when the tumor type and location are favorable. But because we only sample parts of the tissue, we can never be absolutely certain—it’s always about probability, not perfection.
Did You Know?
Waiting for a mass to “declare itself” can turn a simple procedure into a tougher one. As tumors grow, surgeons often need wider margins, which can mean longer anesthesia time, more complex closure, and a larger recovery footprint. Pet parents frequently don’t realize that addressing it earlier can sometimes mean smaller surgery, quicker healing, and potentially lower overall cost—even if it feels counterintuitive at first.