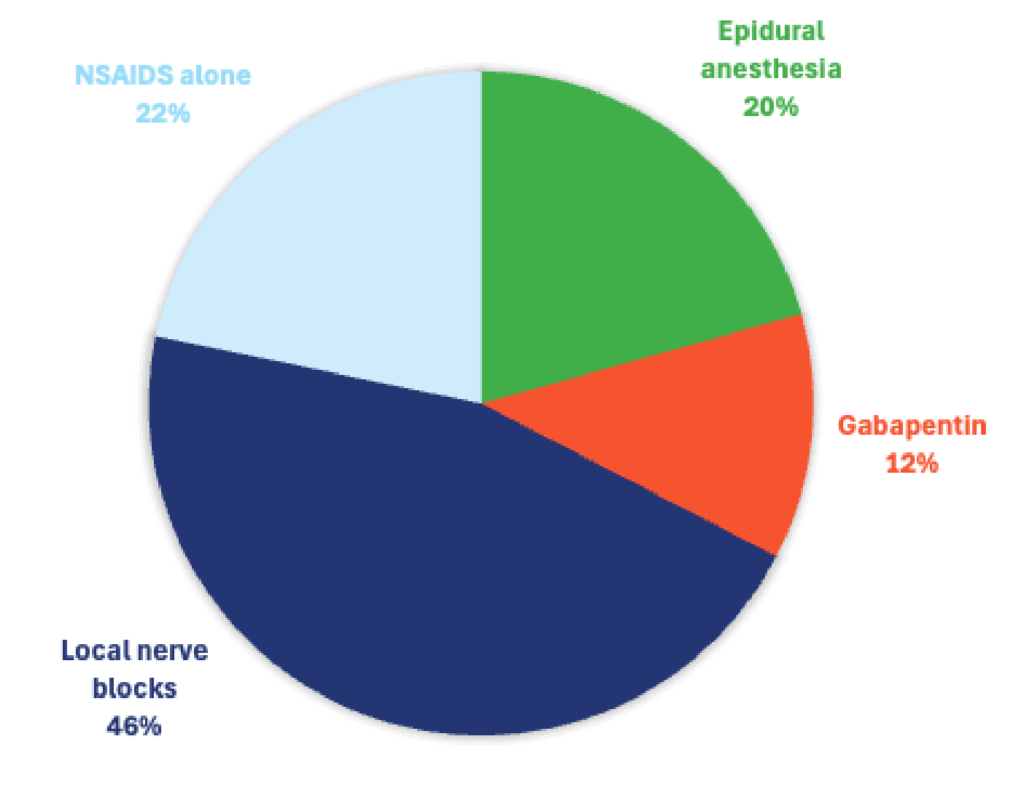
In canine orthopedic surgery, which analgesic modality reduces post-op opioid requirements the most?
- NSAIDS alone
- Epidural anesthesia
- Local nerve blocks
- Gabapentin

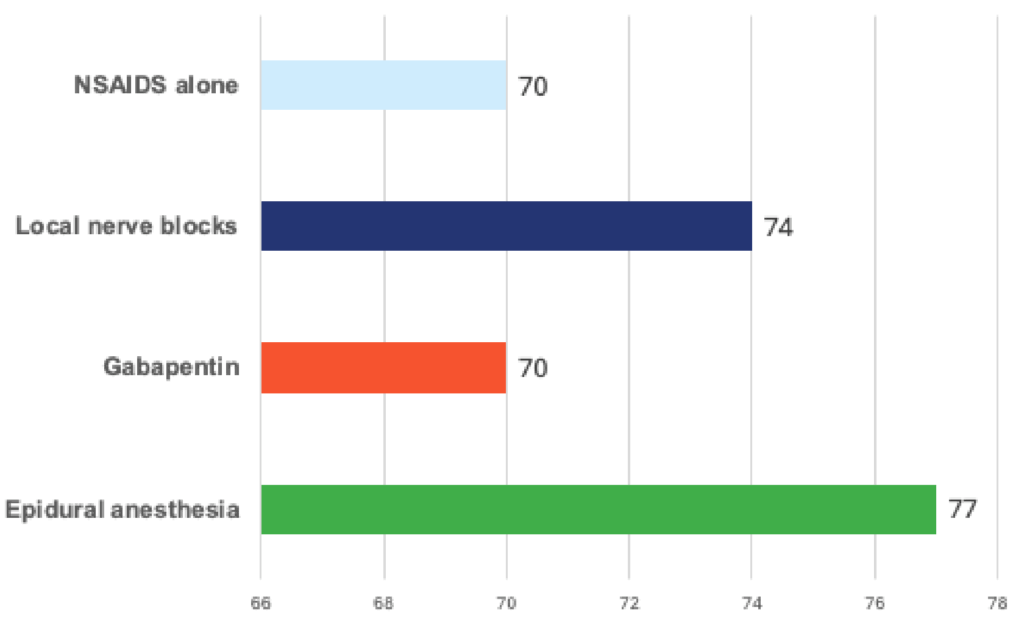
Across the four options provided, locoregional techniques (epidural anesthesia and peripheral/local nerve blocks) are the most consistently associated with marked postoperative opioid sparing in canine orthopedic surgery. When a single “best practice” modality must be selected in isolation, epidural anesthesia is commonly supported as a highly effective option for pelvic limb orthopedic procedures and is frequently characterized as a leading approach in veterinary anesthesia due to its segmental blockade and strong perioperative analgesia.
That said, modern comparative data indicate that femoral–sciatic (and similar) nerve block strategies can provide postoperative analgesia similar to epidural anesthesia for stifle procedures, meaning “best” often depends on local expertise, equipment, and patient-specific considerations rather than a universal hierarchy.
Mechanistic role: NSAIDs reduce pain primarily by inhibiting cyclooxygenase pathways and lowering prostaglandin-mediated peripheral sensitization and inflammation. The AAHA guidelines highlight that NSAIDs expanded access to meaningful perioperative analgesia and remain a foundational therapy in postoperative settings.
Opioid-sparing expectation: NSAIDs are helpful and often reduce overall analgesic burden, but as monotherapy they typically do not blunt nociceptive transmission sufficiently for painful orthopedic procedures. As a result, opioid rescue requirements often remain significant compared with locoregional approaches.
Access/cost considerations: NSAIDs are usually the most accessible and affordable option, but contraindications (renal risk in hypovolemia/hypotension, GI ulceration risk, concurrent steroid use, certain hepatic concerns) can limit their use or require careful case selection.
Clinical positioning: NSAIDs should generally be viewed as a baseline component of multimodal analgesia rather than the primary opioid-sparing “workhorse” for orthopedic surgery when other tools are available.
Mechanistic role: Lumbosacral epidural administration of local anesthetic ± opioid provides segmental blockade of afferent nociceptive transmission at the spinal level, reducing central sensitization and thereby decreasing postoperative analgesic escalation. A prospective randomized blinded clinical study in dogs undergoing pelvic limb orthopedic surgery evaluated epidural morphine vs morphine-bupivacaine combinations for postoperative analgesia, illustrating the established clinical application of epidural opioid and local anesthetic combinations in orthopedic pain control.
Modality review: mechanisms, outcomes, and real-world constraints Opioid-sparing expectation: Epidurals are frequently highly opioid-sparing because they can significantly reduce pain signaling and the need for systemic rescue. In clinical comparisons, epidural anesthesia has demonstrated improvements in postoperative analgesia versus systemic opioid strategies in certain settings.
Access/cost considerations:
Clinical positioning: Epidural anesthesia remains a top-tier modality for pelvic limb orthopedic procedures and, in many hospitals, is the most realistic “high impact” opioid-sparing option when ultrasound-guided peripheral blocks are not consistently available.
Mechanistic role: Peripheral nerve blocks prevent action potential propagation along specific sensory pathways via sodium channel blockade, producing targeted analgesia to the surgical limb while minimizing global systemic drug effects.
Opioid-sparing expectation: Comparative evidence in dogs undergoing stifle joint surgery found that femoral and sciatic nerve blocks provided intraoperative antinociception and postoperative analgesia similar to epidural anesthesia. Additional clinical comparisons in pelvic limb procedures similarly report that epidural anesthesia and certain nerve block techniques can yield similar postoperative analgesia in real-world settings.
Access/cost considerations:
Mechanistic role: Gabapentin modulates neurotransmission via binding the α2δ subunit of voltage-gated calcium channels and is commonly conceptualized as an adjunct for neuropathic pain modulation rather than a primary agent for acute surgical nociception.
Opioid-sparing expectation: Evidence for perioperative gabapentin in veterinary surgical pain is mixed. A study evaluating gabapentin in dogs undergoing TPLO reported that gabapentin (at the studied dose/frequency) did not improve subjective or objective perioperative pain outcomes. Earlier work in dogs in other surgical contexts (e.g., amputation) has investigated gabapentin as an adjunct within a broader analgesic regimen, but it does not consistently emerge as the strongest single “opioid-sparing” modality compared to locoregional anesthesia.
Access/cost considerations:
Clinical positioning: Gabapentin may have a role as an adjunct in select patients, but it is generally not the primary strategy for meaningful opioid reduction after painful orthopedic procedures when locoregional techniques or NSAIDs are available
For the highest level of consistent clinical outcomes in canine orthopedic surgery, the most evidence-aligned approach is multimodal analgesia with a locoregional foundation, supported by anti-inflammatory therapy when appropriate:
Anchor analgesia with a locoregional technique
Layer NSAIDs when medically appropriate
Use opioids as rescue/bridging, not as the primary plan
Reserve gabapentin for specific adjunctive indications
A “best practice” recommendation must acknowledge that real-world implementation varies:
In summary, while epidurals and peripheral blocks represent the most opioidsparing modalities among the listed options, the optimal choice in any hospital depends on training, equipment, patient factors, and client resources, with the best outcomes generally achieved by building a consistent multimodal protocol rather than relying on any single drug.