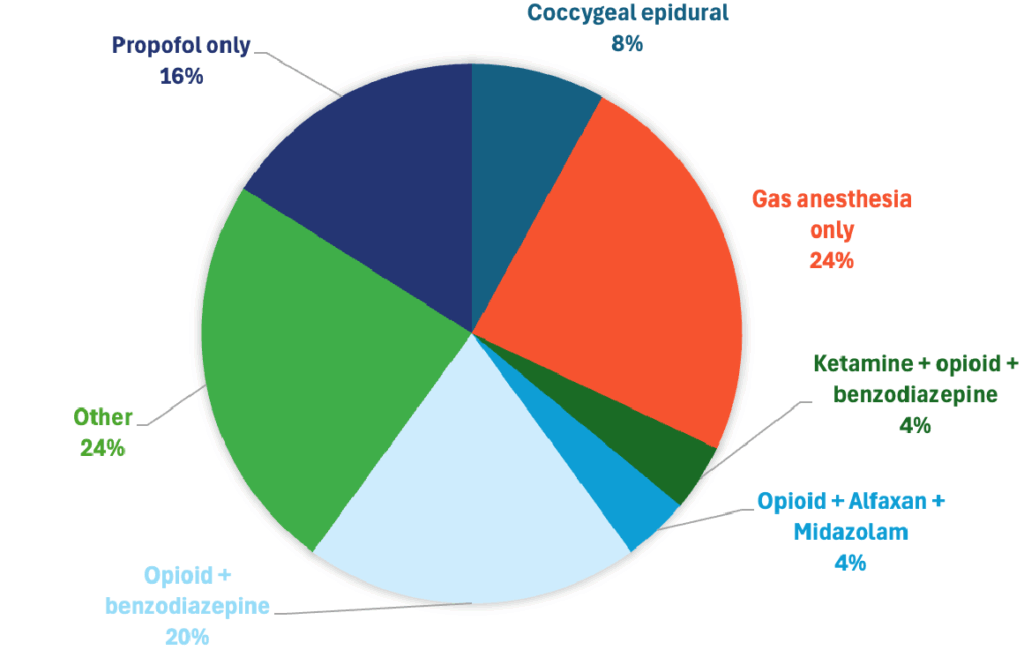
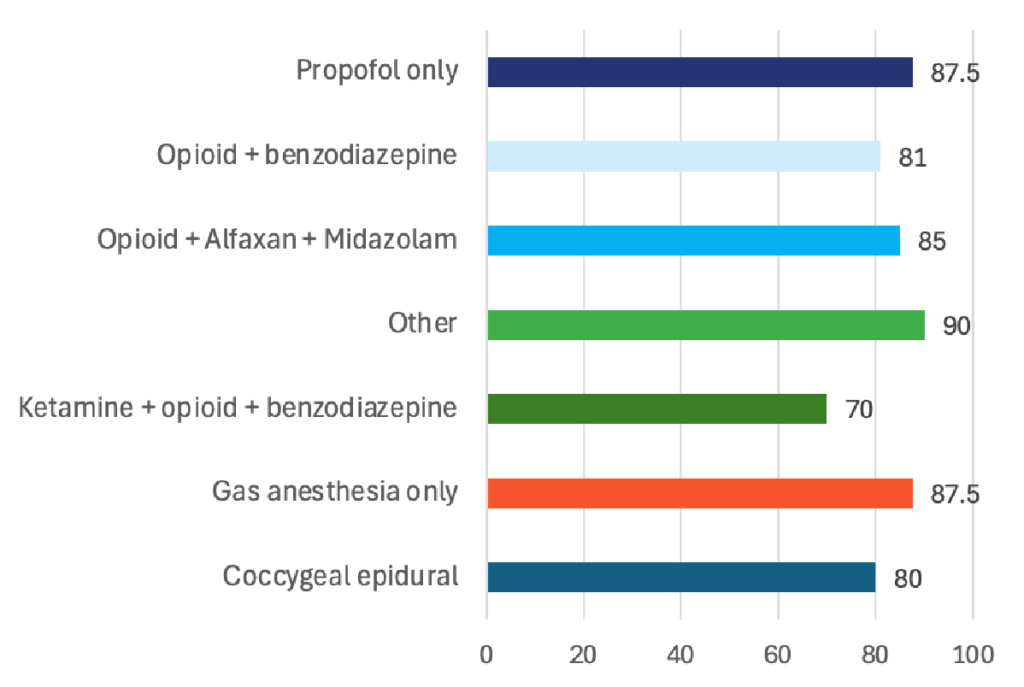
For first-line sedation when unblocking male cats, DVMs most often chose gas anesthesia alone while some chose other forms of sedation not listed. Some preferred propofol only, while others used an opioid paired with a benzodiazepine. Across the board, veterinarians rated these sedation options as very effective, with the most common treatments scoring above 80% effectiveness.

Unblocking a Male Feline
Treatment Selections
Scan to learn more about the coccygeal epidural

Effectiveness
Specialists Insight
Here’s how a board-certified ECC/anesthesia specialist would typically answer when the cat is hemodynamically unstable (e.g., bradycardic from presumed hyperkalemia, azotemic, dehydrated):
First-line choice (for an unstable blocked tom)
Opioid + benzodiazepine, ideally followed (or replaced) by a coccygeal epidural once you have IV access and a brief window of stability.
Why: In shocky or bradyarrhythmic cats, shortacting opioid (e.g., fentanyl or hydromorphone) + benzodiazepine (midazolam/diazepam) yields reliable anxiolysis/analgesia with minimal cardiovascular depression; a sacrococcygeal (caudal) epidural with local anesthetic then provides potent urethral relaxation and analgesia, often allowing catheterization with less systemic anesthesia.
This approach is explicitly recommended in up-todate ECC review guidance and supported by prospective clinical data.
Practical sequence in the truly unstable/bradycardic cat:
- Treat life-threats first (hyperkalemia protocol, small balanced-crystalloid boluses, ECG, calcium gluconate/insulin-dextrose as needed).
- Provide opioid + benzodiazepine for immediate analgesia/sedation.
- Place a coccygeal epidural (lidocaine preferred for rapid onset) to facilitate atraumatic catheterization and reduce systemic drug requirements.
How the specialists would rate each option (for an unstable UO cat)
- Ketamine + opioid + benzodiazepine — Use with caution / not first-line while unstable. Low-dose ketamine combinations are commonly used in stable patients, but ketamine’s renal excretion and potential to increase sympathetic tone/dysphoria make it less desirable until bradyarrhythmias/hyperkalemia are corrected. Consider after stabilization or if other options are unavailable.
- Ketamine + benzodiazepine — Same caveats as above; not first-line in the bradycardic/hyperkalemic patient.
- Opioid + benzodiazepine — Recommended initial chemical restraint for unstable cats (minimal CV depression; benzos perform best in very sick cats). Often all you need to get an epidural placed or to attempt gentle catheterization; supplement with local urethral lidocaine. Top choice among systemic-only options in the decompensated patient.
- Benzodiazepine only — Not sufficient for analgesia or urethral relaxation; can be paradoxical in healthy cats and unreliable alone. Use only as a bridge in the obtunded patient while addressing electrolytes. Opioid only — Helpful for analgesia but often inadequate alone for unobstructing; pair with a benzo and/or regional anesthesia.
- Coccygeal epidural — Strongly recommended (with light sedation). Multiple peer-reviewed reports—including a randomized, double-blinded clinical trial—support caudal epidural (lidocaine or bupivacaine ± preservative-free opioid) to improve catheterization success, reduce systemic anesthetic needs, and provide prolonged analgesia. In unstable cats, this can avoid deeper general anesthesia. Top overall choice when feasible.
- Propofol only — Induction tool, not a protocol. If you must intubate for airway control, titrate propofol very slowly (or consider alfaxalone where available) due to risks of hypotension/apnea in hypovolemic/acidotic cats; use after initial stabilization and monitoring are in place.
- Gas anesthesia only — Not recommended as a sole approach in an unstable/bradyarrhythmic cat (poor control during induction, higher CV/respiratory swings). If used, it should follow preoxygenation, stabilization, and IV access—not as “mask only” without premeds/analgesia.
- Other — Local measures (sterile intraurethral lidocaine gel) and decompressive cystocentesis are valuable adjuncts; alfaxalone is a reasonable alternative induction agent with potentially gentler respiratory effects versus propofol. These are adjunctive to the first-line plan above.
Bottom line (specialist consensus, for the unstable case)
- Treat hyperkalemia and shock first, then
- Opioid + benzodiazepine for immediate, cardio-sparing sedation/analgesia, and
- Coccygeal (caudal) epidural with local anesthetic to achieve urethral relaxation and allow atraumatic catheterization with minimal additional anesthesia.
Subsequently, if deeper anesthesia is needed, carefully titrated propofol/alfaxalone can be used once the patient is more stable.