This is a network committed to advancing clinical understanding through real-world outcomes. We believe veterinarians hold unparalleled insight into what truly works in practice. Each week, we pose one focused clinical question to the veterinary community. On Mondays, we present the question. On Fridays, we share your responses—highlighting the treatments and protocols delivering the best outcomes. Together, we’re building a living library of frontline veterinary wisdom.
Announcing: CareVet Clinical Outcomes Showcase
ALL Veterinary professionals at every level (no licensure required) are encouraged to submit solutions, ideas, innovations, or practices that are meaningfully advancing clinical outcomes – for a chance to earn $5,000.
This Week’s Clinical Question:
Last Week’s Outcomes: Tracheal Collapse
For dogs with suspected tracheal collapse, which management change most improves quality of life?
This week’s audience results skewed toward weight loss and hydrocodone — and our specialists agree with both. Here is why weight loss is the definitive intervention, hydrocodone is its indispensable clinical partner, and the harness is the thing we keep underutilizing.
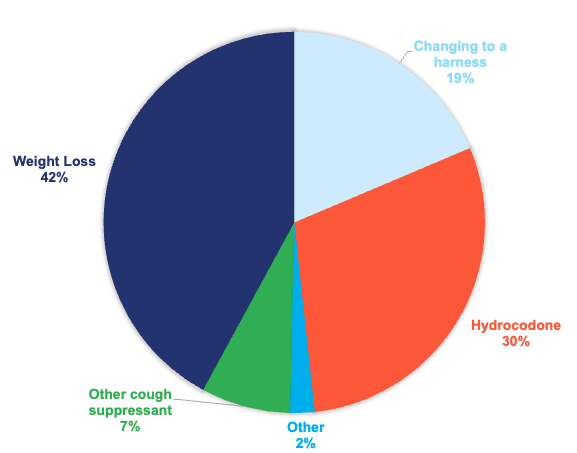
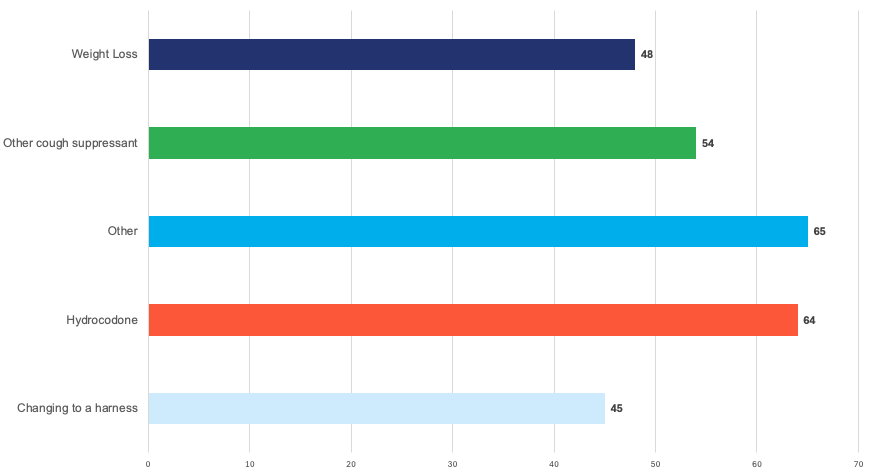
* The pie chart illustrates the percentage of treatments selected by responding DVMs, while the bar chart displays the reported effectiveness of each treatment.
CLINICAL PERSPECTIVE
Tracheal Collapse: Why Weight Loss Is the Answer We Keep Avoiding
RESPIRATORY MEDICINE | QUALITY OF LIFE MANAGEMENT
Weight Loss Is the Answer — And Hydrocodone Is How You Buy Time to Get There
For dogs with suspected tracheal collapse, which management change most improves quality of life?
This week’s clinical question came straight from the field — and for once, the audience largely got it right. When asked which single management change most improves quality of life in dogs with suspected tracheal collapse, responses skewed heavily toward weight loss and hydrocodone. That pattern reflects sound clinical instinct. But instinct and understanding are different things, and understanding why these two interventions lead is what separates a good outcome from a great one.
Weight loss is not a lifestyle recommendation. It is a structural intervention. Hydrocodone is not a long-term solution. It is a bridge. And the harness — which barely registered in this week’s results — is arguably the most underutilized tool in our collective clinical arsenal. Let me walk through each.
No pharmacologic intervention will fully compensate for an airways patient carrying excess body condition. Weight loss is the only management change that addresses the mechanical pathophysiology directly — everything else is symptom management.
PATHOPHYSIOLOGY: WHAT WE ARE ACTUALLY TREATING
Tracheal collapse results from dorsoventral flattening of the tracheal rings due to deficiency or progressive degeneration of C-shaped hyaline cartilage, compounded by laxity of the dorsal tracheal membrane. The result is a dynamically collapsing airway — the trachea narrows during the phase of respiration when intraluminal pressure drops below extraluminal pressure. Cervical tracheal collapse typically worsens on inspiration; intrathoracic collapse on expiration. Many patients present with both components simultaneously.
The clinical presentation is the characteristic paroxysmal, honking cough — often triggered by excitement, heat, exertion, or collar pressure — with variable degrees of dyspnea, exercise intolerance, and cyanosis in severe cases. Critically, the cough itself is both symptom and perpetuating mechanism: each paroxysm inflames already-compromised mucosa, stimulates further afferent cough signaling, and worsens the cycle of airway irritation. This is why antitussive therapy has clinical logic. It is also why addressing the underlying mechanical load — body weight, external compressive forces — has outcomes that pharmacology alone cannot match.
THE SPECIALIST RECOMMENDATION: WEIGHT LOSS FIRST, HYDROCODONE ALONGSIDE
If I have one patient in front of me with tracheal collapse and a body condition score above 6/9, my first prescription is not written on a pad. It is a weight loss protocol. The mechanical burden that excess adipose tissue places on the thorax and airway is continuous, cumulative, and present in every single breath that dog takes. Antitussive therapy reduces cough frequency. Weight loss reduces the force driving the collapse.
The evidence supporting weight reduction in respiratory patients broadly — and in tracheal collapse specifically — demonstrates meaningful improvement in cough frequency, exercise tolerance, and owner-reported quality of life with even modest reductions in body weight. A 10–15% reduction in body weight in an obese tracheal collapse patient can produce clinical improvement that rivals pharmacologic intervention, without the adverse effect profile and without the compliance challenges of chronic medication.
Hydrocodone earns its place as the first-line pharmacologic intervention because the cough cycle is genuinely distressing and self-perpetuating. Breaking it centrally — while the structural management of weight loss, harness transition, and environmental modification takes effect — is clinically rational. It is a bridge, not a destination. Clients who understand this distinction are more likely to commit to the weight management component rather than treating the hydrocodone prescription as the endpoint of care.
Specialist Recommendation Summary
Weight loss is the definitive first-line intervention in any tracheal collapse patient with a body condition score above ideal. Hydrocodone is the appropriate first-line antitussive to manage the cough cycle while structural management takes effect. Harness transition should occur at the first visit in every patient, regardless of severity. These three interventions together form the core protocol — not alternatives to one another.
EVALUATING ALL FIVE OPTIONS
The following reflects the specialist hierarchy for tracheal collapse management, framed against the survey results and grounded in current evidence and clinical consensus.
A
Weight loss
Definitive first-line intervention
This was the historical standard of care and remains appropriate when SIRS criteria are met, when systemic sepsis is suspected, or when the patient fails to improve within 12–24 hours of fluid resuscitation alone. However, routine empirical antimicrobial co-administration in uncomplicated AHDS is not supported by current evidence. Beyond clinical efficacy, antibiotic stewardship is a legitimate concern: unnecessary broad-spectrum therapy disrupts the intestinal microbiome at a time when dysbiosis is already a feature of the presentation, potentially prolonging gastrointestinal recovery and contributing to antimicrobial resistance patterns within the practice population.
B
Hydrocodone
First-line antitussive – essential clinical partner to weight loss
Hydrocodone, as a centrally-acting opioid antitussive, remains the pharmacologic standard of care for tracheal collapse management in North America. Its role is specific and important: to interrupt the self-perpetuating cough cycle while structural interventions take effect. Each cough paroxysm inflames the tracheal mucosa and stimulates further coughing; hydrocodone breaks that afferent signaling loop and reduces the distress that drives client anxiety and owner-reported treatment failure. It should be prescribed with explicit client communication that it is managing symptoms, not the disease — and that weight loss remains the primary therapeutic objective. Sedation and constipation are the most common adverse effects to monitor.
C
Changing to a harness
Immediate, universal – underutilized based on survey results
The survey results here concern me. Harness transition is the lowest-barrier, highest-compliance, zero-adverse-effect intervention available in tracheal collapse management — and it should be initiated at the first visit for every patient regardless of disease grade. Cervical collar pressure generates direct compressive force on the trachea and has been demonstrated to transiently reduce tracheal diameter in susceptible breeds, even during routine leash-walking. Eliminating this mechanical stressor is both immediately actionable and cost-free. The fact that it registered low in this week’s responses suggests it is not receiving the clinical emphasis it deserves. It should be documented, communicated, and reinforced at every appointment.
D
Other Cough Suppressant
Appropriate alternatives when hydrocodone is unavailable or poorly tolerated
Butorphanol is the most clinically comparable alternative to hydrocodone, with a similar antitussive profile and slightly different sedation characteristics that some patients tolerate better. Dextromethorphan is occasionally employed in milder cases, though its evidence base in canine tracheal collapse is less robust than the opioid antitussives. Bronchodilators — terbutaline or theophylline — have a legitimate role when concurrent lower airway disease is identified, as bronchoconstriction compounds dynamic airway obstruction. Short-course corticosteroids at anti-inflammatory doses are appropriate for acute mucosal inflammation and exacerbation management. These agents are useful adjuncts and appropriate alternatives; they do not displace hydrocodone as the first-line antitussive choice in a straightforward presentation.
WHY THE HARNESS RESULT MATTERS
I want to return briefly to the harness data, because I think it reflects a gap worth addressing directly. In a condition where we spend considerable clinical time on pharmaceutical selection and weight counseling, the harness transition is sometimes communicated as an afterthought — mentioned but not emphasized, noted but not documented. It should not be.
The mechanical case for collar elimination is not subtle. We are asking these dogs to breathe through a dynamically collapsing airway while simultaneously applying compressive force to the trachea every time the leash goes taut. Removing that compressive stressor is immediate, costs nothing, requires no compliance beyond a single purchase, and carries no side effects. If we treated it with the same documentation rigor as a prescription, I suspect it would produce measurably better outcomes in the mild-to-moderate population.
A NOTE ON CLIENT COMMUNICATION
The three conversations that most consistently drive outcomes in tracheal collapse management are: (1) a frank, documented weight loss protocol with a target body condition score and a recheck timeline; (2) a clear explanation that hydrocodone is managing symptoms while the real work of weight reduction proceeds; and (3) a harness recommendation delivered as a clinical instruction, not a casual suggestion. Owners who understand the rationale behind each intervention comply at higher rates. Explain the biology. It works.
STAGED MANAGEMENT: HOW THE PROTOCOL BUILDS
For completeness, the following reflects how the intervention hierarchy scales with disease severity. At every grade, weight management and harness transition are non-negotiable. Pharmacologic complexity increases as the disease progresses.
THE CLINICAL TAKEAWAY
Weight loss won this week’s survey because our clinicians have good instincts. Hydrocodone ran close behind because they understand the symptom burden of this disease. What I would ask each of you to take into your next tracheal collapse appointment is not a different answer — it is a clearer explanation of why the answer is what it is, and a renewed commitment to the intervention that gets quietly deprioritized because it is slow and clients push back.
Tracheal collapse is a condition we manage across years, not days. The patients who do best are the ones whose owners understand that weight loss is the treatment, and everything else is support. Make that conversation happen at every visit. Document it. Follow up on it. The airway you protect may not be visible on examination — but it will show up in quality of life.
References
Bauer NB, et al. (2009). Tracheal collapse in dogs. Compendium: Continuing Education for Veterinarians, 31(5), E1–E14.
Johnson LR. (2016). Tracheal collapse: diagnosis and medical and surgical treatment. Veterinary Clinics of North America: Small Animal Practice, 46(2), 513–525.
Tappin SW. (2016). Canine tracheal collapse. Journal of Small Animal Practice, 57(1), 9–17.
White RN. (1995). Surgical management of tracheal collapse in the dog. In Practice, 17, 369–376.
Clinical decisions should always be individualized to patient presentation and practice context.
Clinical Outcomes Annual Report
This report brings together the answers to more than fifteen of this year’s most important clinical questions, offering a comprehensive view of what is working in practices across the country.
Subscribe today and become part of the Clinical Outcomes Network.
Check Out Past Results
See how veterinarians nationwide answered previous Clinical Outcomes questions and what their results reveal.
2 Comments. Leave new
Love the result/pie chart!
Excellent resource